BackgroundLinear enamel hypoplasia (LEH) and porous cranial lesions such as cribra orbitalia (CO) and porotic hyperostosis (PH) are considered nonspecific indicators of early childhood metabolic stress.
ObjectivesThe study aims to describe the association of LEH with CO and PH in a sample of the Kirsten Skeletal Collection (KSC) representing a cohort in the Western Cape, South Africa. This will be used to determine if one or more of these lesions can be used as an indicator of adult mortality.
Sample and MethodsSkulls (n = 412) of both sexes with known demographics from the KSC were macroscopically scored for LEH, CO and PH lesions using a ring light. This study was ethically approved by the Health Research and Ethics Committee of Stellenbosch University (S13/05/100).Statistical chi-square tests were used to determine the association between lesions and student’s t-tests to determine if there was a significant difference in mean age-of-death between groups.
ResultsThere was no association when comparing LEH with CO and PH in the cohort, although an association was found between CO and PH. Individuals who exhibited the pathological lesions for LEH, CO or PH (or a combination thereof) were observed to have a younger mean age-at-death than the individuals without any of the three disease lesions.
ConclusionsThe lesions may potentially be used as an indicator of adult mortality. However, the results of this study might represent a biased population of low socio-economic status in the Western Cape as represented in the KSC, rather than the general population of the region.
Conflict of interest: There are no conflicts of interest.
Citation: Marais, C. et al. (2022). The association between linear enamel hypoplasia, cribra orbitalia and porotic hyperostosis in a South African skeletal sample. Human Biology and Public Health 2. https://doi.org/10.52905/hbph2023.2.71.
Copyright: This is an open access article distributed under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Pathological lesions observed on skeletal remains can provide valuable information to determine childhood physiological stresses and the standard of living of a population.
Contents
Introduction
Skeletal lesions on human remains are a direct product of interactions between biological, social and environmental factors. A number of skeletal indicators of metabolic disorders, nutritional deficiencies and hormonal disturbances with which to assess the nutritional status of a population, can be observed on bone (Ortner 2003). Metabolic disorders of bone are disorders in which a bone mass reduction results from insufficient osteoid production or excessive bone de-ossification (White et al. 2012). These disorders may be due to malnutrition, which may include inadequate intake of nutrients or insufficient absorption of ingested nutrients (Ortner 2003).
During childhood and adolescence, the diploe of the cranial vault and medullary cavities of the long bones are the primary sites for erythropoiesis, and therefore juveniles are more likely to exhibit skeletal lesions associated with anaemia and other physiological stresses (Blom et al. 2005; Brickley 2018; Walker et al. 2009). Anaemic stress can cause an increase in erythrocyte production leading to hypertrophy and hyperplasia of the haemopoietic bone marrow and diploe (Mensforth et al. 1978). In long bones, anaemias are observed as metaphyseal widening and cortical thinning. However, in flat bones it presents as cranial bone thickening, coarsening of the trabeculae, and widening of the diploe.
Iron deficiency anaemia lesions such as cribra orbitalia (CO) are visible as pitting (small holes) in the outer layer of bone in the roof of the orbits (Brickley 2018; Ortner 2003; Walker et al. 2009). A number of factors have been implicated in causing CO, many of which are under debate, for example iron deficiency anaemia, sickle cell anaemia, malnutrition, scurvy, chronic gastrointestinal bleeding, ancylostomiasis and epidemic disease (Brickley 2018; Oxenham and Cavill 2010; Rivera and Mirazón Lahr 2017; Walker et al. 2009).
Porotic hyperostoses (PH) are lesions which manifest as areas of porosity on the outer table and diploe of the frontal, parietal, and occipital bones of the cranium accompanied by increased vault thickness (Brickley 2018; Merwe 2007; Walker et al. 2009). Although these lesions are similar to CO, the disease process is much more severe and is associated with major iron deficiency anaemia (Brickley 2018; Ortner 2003; Walker et al. 2009). In children, the bone can be thickened with large foramina, while in adults only remnants of the holes (frequently only pits) remain. Lesions seen in adults result from bone changes occurring in the growth period that have not undergone complete remodelling (Kozak and Krenz-Niedbała 2002; Merwe 2007; Stuart-Macadam 1987).
Dental enamel forms during juvenile growth and, in contrast to bone, never remodels after its formation. When dental enamel formation is disrupted, resulting in a reduction of enamel thickness (Goepferd and Flaitz 1981) due to metabolic insult, defects can occur in the tooth enamel structure (White et al. 2012). Linear enamel hypoplasia (LEH), also referred to as dental enamel hypoplasia or simply as dental hypoplasia, is a nonspecific quantitative enamel defect, presenting as three main forms of defects on teeth, as classified by Lukacs (1989): a) linear horizontal grooves, b) linear/non-linear pits, and c) linear grooves and pits in the tooth crown enamel as a result of defects in ameloblastic activity. This dental defect represents a short period when growth slowed down or stopped during the formation of the tooth crown (the foetal period) until the age of eruption of the last tooth (Goodman and Rose 1990; Steckel and Rose 2002). Robinson et al. (1983) have stated that the exact aetiology of LEH cannot be specified, but likely factors that may result in LEH are periapical inflammation or trauma to a deciduous tooth, fever, disease, nutritional deficiencies endocrine dysfunction, and generalised infection during odontogenesis. Due to these varied aetiological causes, LEH is considered a nonspecific indicator of human population health (Goodman and Armelagos 1988; Huss-Ashmore et al. 1982).
The aim of this study is to describe the association of LEH with CO and PH in the Kirsten Skeletal Collection (KSC) and thereby to determine if one or more of these lesions can be used as an indicator of adult mortality.
Sample & Methods
Sample
The Kirsten Skeletal Collection (KSC) is a registered skeletal biobank (B20/09/004) housed in the Division of Clinical Anatomy, Faculty of Medicine and Health Sciences at Stellenbosch University in South Africa. The KSC contains skeletal specimens obtained mainly from cadavers with known records, used for the training of medical students at the University (Labuschagne and Mathey 2000; Alblas et al. 2018). Under the Human Tissue Act 65 (South African National Department of Health 1983), the more recent National Health Act 61 (South African National Department of Health 2004) and the protection of the regional Inspector of Anatomy, Stellenbosch University is allowed to receive cadavers for both teaching and research purposes. The KSC represents a population who lived between the mid- and late 20th century, as most of the individuals were born between 1920 and 1949 (42%) and died between 1970 and 1989 (54%) (Alblas et al. 2018; Pfeiffer et al. 2016). The KSC has been reported to have an overrepresentation of males, aged individuals, and people with lower socio-economic status (Alblas et al. 2018).
This study was ethically approved by the Health Research and Ethics Committee (HREC) of Stellenbosch University (S13/05/100). The skeletal remains of 412 individuals from the KSC, were analysed for the purpose of this study. Individuals were chosen according to their completeness, and those with severe damage or trauma to the crania were excluded from the sample. Skeletons with known cadaver records with information concerning their sex, age-at-death, population affinity, and cause of death were used for analysis. Cause of death and general frailty of the skeleton were taken into account when collecting and processing the data, although both factors were not used as predictors (of mortality) in this study.
Methods
According to Goodman et al. (1988), the two maxillary incisors and the two mandibular canines are to be used for scoring the presence of LEH in the teeth. However, in this study, many individuals did not have incisors to analyse. Modification and extraction of partial or full dentition were normal for inhabitants of the Western Cape during the 20th century (Alblas et al. 2018; Friedling and Morris 2007). Therefore, all available dental elements on the maxillae and mandibles were macroscopically assessed for the presence of LEH. A dental probe was used to manually detect any sign of growth-arrest lines or pits in the crown enamel of a tooth. Enamel hypoplasia was marked as ‘Present’ if at least one defect in the tooth enamel (horizontal lines or pitting) was visible, whilst teeth showing no defects were scored as ‘Absent’. No attempt was made to record the position of the lesion on the surface of the crown, and the number of lines per tooth was not counted.
Porotic hyperostosis was observed as porosity on the external cranial vault and CO as porosity in the orbital roof (Facchini et al. 2004; Walker et al. 2009). Any sign of pitting with accompanying vault thickness on the frontal, parietal and/or occipital surfaces was scored positively for each individual (Stuart-Macadam 1985), and an expanded diploe was also considered. So, the lesions were scored as ‘Present’ in the individual for all severity grades of PH and CO outlined in the grading system of Buikstra and Ubelaker (1994). Post-mortem damage due to storage erosion and handling of artefacts were considered when the lesions were analysed, with the use of a magnifying ring light.
Statistical Analysis
Contingency tables were created to determine the frequency of LEH prevalence across both sexes, as well as CO and PH presence. Descriptive statistics including mean and standard deviation were calculated for age-at-death for each category. Pearson’s chi-squared test and Fisher’s exact test were used to identify the significance of the associations between categorical variables. A Shapiro-Wilk test was used to assess the normality distribution of age-at-death across the sample. The differences in average age-at-death for individuals with or without LEH were determined by using a Student’s t-test. For all tests, a significance level of p < 0.05 was used. All statistical analyses were performed using RStudio software version 4.2.1.
Results
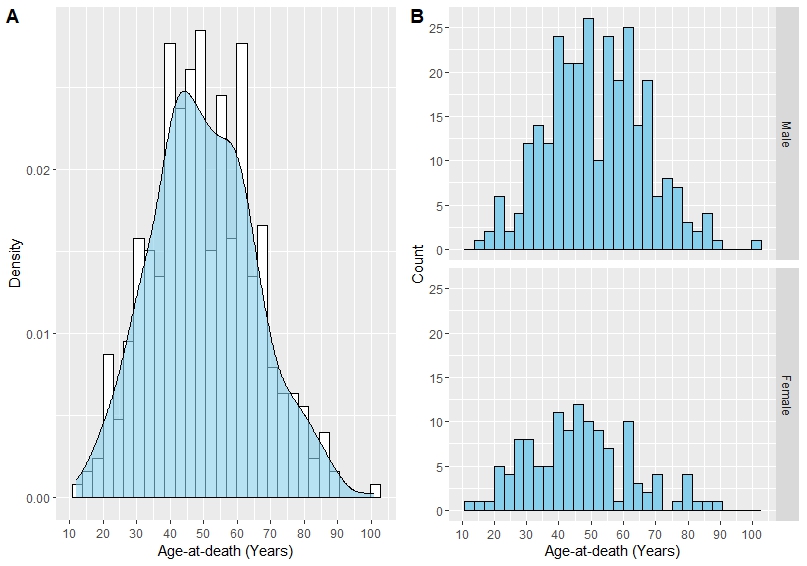
The sample consisted of 412 individuals ranging from 12 to 101 years of age. As illustrated in Figure 1A, the age-at-death was normally distributed across the total sample. The proportion of males in the sample was noticeably larger compared to females, with the male-to-female ratio calculated at 2.3:1 (Figure 1B).
Figure 1 Frequency distribution of age-at-death in the sample displayed a normality curve. A) Normal distribution of ages across total sample (ungrouped) and B) within male and females (grouped). Figures are generated in RStudio (R Core Team 2022).
Figure 2 Visual depiction of the disease lesions observed in the sample. A) Linear enamel hypoplasia on left mandibular incisors and canine, B) cribra orbitalia in the left orbital roof, and C) porotic hyperostosis on left parietal bone. Photographs by Chantelle Marais, 2022.
Examples of LEH, CO and PH in the sample can be seen in Figure 2. The frequency distribution and statistical analysis of LEH with sex, CO and PH is summarised in Table 1. Figure 3 illustrates the frequency of males and females with LEH in co-occurrence with CO and PH. Enamel hypoplasia was observed in a total of 35 (8.5%) of the skeletons assessed. Due to the lack of teeth in the present population, this may not be an accurate representation of the number of LEH cases in the skeletal population. Linear enamel hypoplasia had a higher prevalence in males (n = 22) than in females (n=13), although this was not significant (p > 0.05). Of the total skeletons with LEH, only 2.2% (n = 9) showed signs of CO as well. In the absence of LEH, CO occurred in 12.4% (n = 51) of the individuals, whereas PH occurred in 15.5% (n = 64) of individuals with no LEH. Results for the Fisher’s Exact test revealed that there was no statistically significant association between the occurrence of LEH with either CO (p = 0.075) or PH (p = 0.816).
Figure 3 Prevalence of LEH in males and females with co-occurrence of A) cribra orbitalia and B) porotic hyperostosis. Figures are generated in RStudio (R Core Team 2022).
Table 1 Frequency distribution and statistical analysis of Linear Enamel Hypoplasia, with Sex, Cribia Orbitalia and Porotic Hyperostosis variables in the Kirsten Skeletal Collection (KSC), Stellenbosch, South Africa.
Linear enamel hypoplasia
P-value
Effect size (Phi)
Absent
Present
Total
Pearson's chi-sq
Fisher's exact
Sex
Male
266 (64.6%)
22 (5.3%)
288 (69.9%)
0.342
0.341
0.05
Female
111 (26.9%)
13 (3.2%)
124 (30.1%)
Total
377 (91.5%)
35 (8.5%)
412 (100%)
Cribra orbitalia
Absent
326 (79.1%)
26 (6.3%)
352 (85.4%)
0.051
0.075
0.1
Present
51 (12.4%)
9 (2.2%)
60 (14.6%)
Total
377 (91.5%)
35 (8.5%)
412 (100%)
Porotic hyperostosis
Absent
313 (76.0%)
30 (7.3%)
343 (83.3%)
0.683
0.816
-0.02
Present
64 (15.5%)
5 (1.2%)
69 (16.7%)
Total
377 (91.5%)
35 (8.5%)
412 (100%)
However, a statistically significant association was observed between CO and PH (p < 0.0001), with both lesions scored as ‘Present’ in 35 (8.50%) of the total 412 crania examined (Table 2). Within the sample, 34 of the 69 individuals with PH did not present with CO, whereas 25 of the 60 individuals with CO did not show signs of PH.
Table 2 Contingency table showing the frequencies and associations of Cribia Orbitalia and Porotic Hyperostosis in the Kirsten Skeletal Collection (KSC), Stellenbosch, South Africa.
Porotic hyperostosis
Pearson's chi-sq
Effect size (Phi)
Absent
Present
Total
X2
df
p
Cribra orbitalia
Absent
318
34
352
83.65
1
p < 000.0
0.46
(77.18%)
(8.25%)
Present
25
35
60
(6.07%)
(8.50%)
Total
343
69
412
Regarding the age-at-death analyses, it was noted that the average age recorded for individuals with LEH was generally lower compared to those who did not present with LEH (Table 3). When considering sex as a variable in addition to LEH presence, both males and females presenting with LEH died at a younger age. For males, the mean age-at-death was calculated at 9.79 years younger for those with LEH, whilst females died approximately 13 years younger when showing signs of LEH (Table 3). The differences in mean age-at-death within male and female groups showing signs of LEH were significant (t-test: p < 0.05) and is illustrated with the use of boxplots in Figure 4.
Figure 4 Boxplots showing the distribution of age-at-death in males and females with LEH. The differences in average age-at-death for individuals with or without LEH was determined by using a Student’s t-test. ). Figures are generated in RStudio (R Core Team 2022)
Table 3 Mean, median and standard deviation for adult age-at-death in Linear Enamel Hypoplasia (LEH) by other variables such as sex, Cribia Orbitalia (CO), and Porotic Hyperostosis (PH) in the Kirsten Skeletal Collection (KSC), Stellenbosch, South Africa.
Variable
n
Mean
Median
sd
LEH Absent
PH Absent
313
52.22
51
15.55
PH Present
64
45.09
45.5
12.21
LEH Present
PH Absent
30
40.60
41
14.62
PH Present
5
32.60
33
10.45
LEH Absent
CO Absent
326
51.65
50
15.64
CO Present
51
46.90
45
11.93
LEH Present
CO Absent
26
39.23
41
14.25
CO Present
9
40.11
34
15.14
LEH Absent
Male
266
52.38
51
14.99
Female
111
47.74
47
15.48
LEH Present
Male
22
42.59
41.5
12.20
Female
13
34.15
28.0
16.34
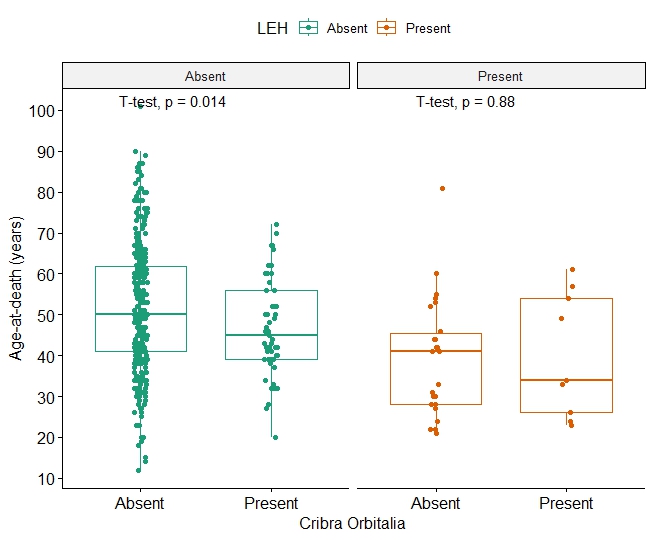
After grouping the sample according to LEH presence/absence, it was noted that individuals with both LEH and CO died at a mean age of 40.11 ± 15.14 years (Table 3). Individuals with LEH but no CO died at an average age of 39.23 ± 14.25 years (Table 3). This difference between the mean ages had a p-value of 0.88 and was therefore not significant (Figure 5). Meanwhile, within the ‘LEH Absent’ group, individuals with CO died at a younger mean age (46.90 ±11.93 years) than those who showed no signs of either LEH or CO (51.65 ± 15.64 years). The difference between these mean ages was found to be significant (p = 0.014) (Figure 5).
Figure 5 Boxplots demonstrating the distribution of age-at-death with LEH and CO. Individuals were grouped according to LEH presence/absence. For each group, the differences in average age-at-death for individuals with or without CO was determined by using a Student’s t-test. Figures are generated in RStudio (R Core Team 2022).
A similar trend was observed with the age-at-death analyses when considering LEH presence in addition to the prevalence of PH. Individuals with LEH but not PH experienced a slightly longer lifespan of 40.60 ± 14.62 years compared to the 32.60 ± 10.45 years for individuals presenting with both LEH and PH lesions (Table 3), although this finding was not significant (p = 0.18) (Figure 6). A significant difference (p < 0.05) between the average age-at-death for those with or without PH was observed within the ‘LEH Absent’ group (Figure 6).
Figure 6 Boxplots illustrating the distribution of age-at-death with LEH and PH. Individuals were grouped according to LEH presence/absence. For each group, the differences in average age-at-death for individuals with or without PH was determined by using a Student’s t-test. Figures are generated in RStudio (R Core Team 2022).
Discussion
The study aimed to describe the association of linear enamel hypoplasia (LEH) with cribra orbitalia (CO) and porotic hyperostosis (PH) in the Kirsten Skeletal Collection (KSC) and thereby determine if one or more of these lesions can be used as an indicator of adult mortality.
Prevalence and association of early physiological stress markings in the KSC
In population-specific studies, the prevalence of LEH in different populations varies between 3.0% (Seow et al. 1987) in developed countries or well-nourished populations, to 99.0% (Pascoe and Seow 1994) in developing countries or populations living under low socio-economic conditions (Goodman et al. 1980; Malville 1997; Saunders and Keenleyside 1999). Genetic factors, as well as exposure to similar environmental stresses, can have an influence on the susceptibility of LEH. For example, a study on young Australian Aboriginal children from Bathurst Island (Pascoe and Seow 1994), showed a prevalence of 99.0% LEH, with nearly all the patients presenting with a full range of medical problems from similar environmental stressors. A similar study on Guatemalan children, however, showed a significantly higher prevalence of LEH among siblings, while the general prevalence of LEH in the population fell between 18.0% and 24.0% (Infante and Gillespie 1974), in this instance suggesting a genetic influence.
The prevalence of LEH in the present study was recorded in 35 (8.5%) of the 412 individuals analysed. The KSC comprises of individuals who lived between the mid- and late 20th century with low socio-economic conditions and poor access to health care (Labuschagne and Mathey 2000; Pfeiffer et al. 2016). These communities also showed a high prevalence of pulmonary infectious diseases, such as pneumonia and tuberculosis (Geldenhuys 2014), and a high prevalence of infectious diseases (Alblas et al. 2018) that may contribute to the formation of LEH (Aufderheide and Rodríguez-Martín 1998). Therefore, a higher number of LEH was expected. The low prevalence of LEH observed in the current sample may be due to the lack of dentition available for analysis and the result is not a true representation of the signs of LEH in the individuals in the KSC.
The results of this study showed no statistical significance between LEH presence and sex; however, the prevalence in males is slightly higher than in females. Most studies comparing sexes showed no difference in the prevalence of LEH (Infante and Gillespie 1974; Kozak and Krenz-Niedbała 2002; Malville 1997). Studies conducted by Li et al. (1995) as well as Saunders and Keenleyside (1999) showed a statistically higher prevalence of LEH in males than in females, supporting the theory that males are more sensitive to external environmental effects during growth than females. In a review by Stinson (1985) on sex differences to environmental sensitivity, it was concluded that this theory is difficult to prove in the postnatal period due to complex environmental differences and cultural differences between population groups. Prenatal differences in environmental sensitivity show more consistent trends with males showing a higher mortality rate than females prenatally (Stinson 1985). The same study also showed that maternal nutritional supplementation improved growth in males more than in females (Stinson 1985).
The current study did not show a significant association between the presence of LEH with the presence of either CO or PH. CO and PH can occur both during adult- and childhood, although the lesions (especially CO) are more apparent in children (Walker et al. 2009). Lesions of CO and PH are believed to be related. Previous authors have suggested that bony lesions usually start in the orbits and then if metabolic stress continues, spread to the parietal and occipital bones due to a difference in diameter and microstructure of the bones (Facchini et al. 2004; Stuart-Macadam 1985; Wapler et al. 2004). Anaemic stress can cause an increase in erythrocyte production leading to hypertrophy and hyperplasia of the haemopoietic bone marrow and diploe (Mensforth et al. 1978). Porotic hyperostosis is usually associated with CO while CO frequently occurs without PH (Lallo et al. 1977). The present study found that 35 of the 412 individuals (8.5%) showed signs of both CO and PH. Of the total sample, 34 of the 69 individuals with PH did not present with CO, whereas 25 of the 60 individuals with CO did not show signs of PH. The results for the correlation analysis between CO and PH was significant.
In most studies, females showed a higher prevalence of signs of anaemia (collectively seen as CO and PH) than males (Bharati and Basu 1990; Kozak and Krenz-Niedbała 2002; Wapler et al. 2004; Webb 1982). The reason for this lies in the physiology of a female who, during, for example, menstruation, childbirth, and lactation loses iron (Kozak and Krenz-Niedbała 2002). Rosso and Lederman (1982) suggested that developing countries, like South Africa, have an anaemic bias towards young females due to a tendency for pregnancies at a young age, malnutrition, and poor access to healthcare facilities. Furthermore, males have a larger iron storage ability than females due to slower growth in late adolescence, thereby improving their iron level status, thus females are more likely to exhibit signs of iron deficiency anaemia than males (typically). This contradicts the findings of the present study which showed a higher prevalence of CO and PH in males than in females, although this finding was not significant. Only a few other studies found a higher prevalence in males but none of them with significant differences (Facchini et al. 2004; Fairgrieve and Molto 2000). This suggests that a factor other than anaemia may have contributed to CO and PH. Other factors previously suggested include post-mortem erosion, hyper-vascularisation, osteoporosis and osteitis (Wapler et al. 2004).
Age-at-death analysis
It has been hypothesised that individuals with more stress episodes during childhood are more prone to higher morbidity and early mortality. In an attempt to understand whether these early physiological stress markers can provide insight to the expected adult mortality in the KSC, the age-at-death of the individuals who exhibited any one of the three lesions (LEH, CO or PH) were compared in terms of their average age to all the individuals who did not exhibit one of the three pathological lesions.
In general, the individuals in this study who exhibited the pathological lesions for LEH, CO or PH had a younger mean age-at-death than the individuals without any of the three lesions. This stands in contrast to results from previous studies in which the authors did not find any correlation between age-at-death and LEH (Saunders and Keenleyside 1999). A possible explanation for the decrease in LEH may be that the children developing this defect were exposed to infections and malnutrition not just during childhood but throughout life resulting in death at an earlier age. The individuals without the defect were most likely better nourished and lived under better socio-economic conditions, thereby decreasing the opportunity of obtaining infectious diseases to a similar extent.
The results of the current study showed that LEH, PH and CO may be used (separately) as an indicator for adult age-at-death, but not necessarily in combination. One should also note that porous lesions like CO, often have a more complicated aetiology, such as subperiosteal reactions associated with nutritional deficiencies, and complicated by a high alcohol intake (Mensforth et al. 1978; Steckel and Rose 2002). Non-specific infectious diseases, among other causes, play a more prominent role in the aetiology of subperiosteal bone reactions, which can occur throughout life (Brickley 2018; Ortner 2003). Due to the lack of access to medical records of the individuals in this sample, the usefulness of the disease lesions as indicators of a healthy or diseased society are not exact and cannot be referenced to the social context of the society. In light of the Osteological Paradox (Wood et al. 1992), these disease lesions' interpretations can be twofold. On one side, they might signify a population which endured numerous health challenges, portraying a frail demographic. On the contrary, they could represent a resilient group that endured health problems long enough for the lesions to manifest on the skull.
Further speculation as to possible specific causes of the observed lesions of CO and PH within the sample was not attempted, as the severity and state (active or healed) of the lesions were not taken into account during data collection. Other disease conditions observable from the skeletal remains were also excluded from the current study and could thus be useful to include in future studies.
Conclusion
In the present study, a slightly higher prevalence of LEH, CO, and PH was observed in males than in females. Even though these differences were not statistically significant, they may suggest that males were under more environmental and other stresses than females during childhood. Individuals who exhibited the pathological lesions for LEH, CO, or PH (or a combination thereof) were observed to have a younger mean age-at-death than the individuals without any of the three lesions. Thus, the lesions may potentially be used as an indicator of adult mortality. The results of this study might represent a biased population of low socio-economic status in the Western Cape, rather than the general population of the region (Labuschagne and Mathey 2000; Pfeiffer et al. 2016).
Acknowledgements
This manuscript and statistical analysis were the result of the participation in the 5th International Summer School of the University of Potsdam, which took place in July 2022. The authors would like to thank PD Dr. Christiane Scheffler, Dr. Detlef Groth, and Prof. Michael Hermanussen for this opportunity as well as for their patience and assistance during the summer school. We appreciate the generous funding by KoUp.
References
Alblas, A./Greyling, L. M./Geldenhuys, E.-M. (2018). Composition of the Kirsten Skeletal Collection at Stellenbosch University. South African Journal of Science 114 (1/2). https://doi.org/10.17159/sajs.2018/20170198.
Aufderheide, A. C./Rodríguez-Martín, C. (1998). The Cambridge encyclopedia of human paleopathology. Cambridge, Cambridge University Press.
Bharati, P./Basu, A. (1990). Fertility, mortality and maternal anaemic status in a village population of West Bengal, India. Annals of Human Biology 17 (4), 331–335. https://doi.org/10.1080/03014469000001102.
Blom, D. E./Buikstra, J. E./Keng, L./Tomczak, P. D./Shoreman, E./Stevens-Tuttle, D. (2005). Anemia and childhood mortality: latitudinal patterning along the coast of pre-Columbian Peru. American Journal of Physical Anthropology 127 (2), 152–169. https://doi.org/10.1002/ajpa.10431.
Brickley, M. B. (2018). Cribra orbitalia and porotic hyperostosis: a biological approach to diagnosis. American Journal of Physical Anthropology 167 (4), 896–902. https://doi.org/10.1002/ajpa.23701.
Buikstra, J. E./Ubelaker, D. H. (Eds.) (1994). Standards for data collection from human skeletal remains. Proceedings of a seminar at the Field Museum of Natural History, organized by Jonathan Haas. Fayetteville, AR, Arkansas Achaeological Survey.
Facchini, F./Rastelli, E./Brasili, P. (2004). Cribra orbitalia and cribra cranii in Roman skeletal remains from the Ravenna area and Rimini (I–IV century AD). International Journal of Osteoarchaeology 14 (2), 126–136. https://doi.org/10.1002/oa.717.
Friedling, L. J./Morris, A. (2007). Pulling teeth for fashion: dental modification in modern day Cape Town, South Africa. South African Dental Journal 62 (3), 106–113.
Geldenhuys, E.-M. (2014). A morphological assessment of the health status of a cadaver population at the Faculty of Health Sciences, Stellenbosch University, with special reference to tuberculosis (TB) lesion distribution. PhD Thesis. Stellenbosch University. Available online at http://hdl.handle.net/10019.1/95764 (accessed 12/14/2023).
Goepferd, S. J./Flaitz, C. M. (1981). Enamel hypoplasia associated with congenital hypoparathyroidism. Pediatric Dentistry 3 (2), 196–200.
Goodman, A. H./Armelagos, G. J. (1988). Childhood stress and decreased longevity in a prehistoric population. American Anthropologist 90 (4), 936–944. https://doi.org/10.1525/aa.1988.90.4.02a00120.
Goodman, A. H./Armelagos, G. J./Rose, J. C. (1980). Enamel hypoplasias as indicators of stress in three prehistoric populations from Illinois. Human Biology 52 (3), 515–528.
Goodman, A. H./Rose, J. C. (1990). Assessment of systemic physiological perturbations from dental enamel hypoplasias and associated histological structures. American Journal of Physical Anthropology 33 (S11), 59–110. https://doi.org/10.1002/ajpa.1330330506.
Goodman, A. H./Thomas, R. B./Swedlund, A. C./Armelagos, G. J. (1988). Biocultural perspectives on stress in prehistoric, historical, and contemporary population research. American Journal of Physical Anthropology 31 (S9), 169–202. https://doi.org/10.1002/ajpa.1330310509.
Huss-Ashmore, R./Goodman, A. H./Armelagos, G. J. (1982). Nutritional inference from paleopathology. In: M. B. Schiffer (Ed.). Advances in archaeological method and theory. New York/London, Academic Press, 395–474.
Infante, P. F./Gillespie, G. M. (1974). An epidemiologic study of linear enamel hypoplasia of deciduous anterior teeth in Guatemalan children. Archives of Oral Biology 19 (11), 1055–1061. https://doi.org/10.1016/0003-9969(74)90095-8.
Kozak, J./Krenz-Niedbała, M. (2002). The occurrence of cribra orbitalia and its association with enamel hypoplasia in a medieval population from Kołobrzeg, Poland. Variability and Evolution 10, 75–82.
Lallo, J. W./Armelagos, G. J./Mensforth, R. P. (1977). The role of diet, disease, and physiology in the origin of porotic hyperostosis. Human Biology 49 (3), 471–483.
Li, Y./Navia, J. M./Bian, J.-Y. (1995). Prevalence and distribution of developmental enamel defects in primary dentition of Chinese children 3–5 years old. Community Dentistry and Oral Epidemiology 23 (2), 72–79. https://doi.org/10.1111/j.1600-0528.1995.tb00204.x.
Lukacs, J. R. (1989). Dental paleopathology: methods for reconstructing dietary patterns. In: M. Y. İşcan/K. A. R. Kennedy (Eds.). Reconstruction of life from the skeleton. New York, Alan R. Liss, 261–286.
Mensforth, R. P./Lovejoy, C. O./Lallo, J. W./Armelagos, G. J. (1978). Part two: the role of constitutional factors, diet, and infectious disease in the etiology of porotic hyperostosis and periosteal reactions in prehistoric infants and children. Medical Anthropology 2 (1), 1–59. https://doi.org/10.1080/01459740.1978.9986939.
Merwe, A. E. van der (2007). Human skeletal remains from Kimberley: an assessment of health in a 19th century mining community. MSc Thesis. University of Pretoria. Available online at http://hdl.handle.net/2263/26172 (accessed 11/29/2023).
Ortner, D. J. (2003). Identification of pathological conditions in human skeletal remains. 2nd ed. Amsterdam, Academic Press.
Oxenham, M. F./Cavill, I. (2010). Porotic hyperostosis and cribra orbitalia: the erythropoietic response to iron-deficiency anaemia. Anthropological Science 118 (3), 199–200. https://doi.org/10.1537/ase.100302.
Pascoe, L./Seow, W. K. (1994). Enamel hypoplasia and dental caries in Australian aboriginal children: prevalence and correlation between the two diseases. Pediatric Dentistry 16 (3), 193–199.
Pfeiffer, S./Heinrich, J./Beresheim, A. (2016). Cortical bone histomorphology of known-age skeletons from the Kirsten collection, Stellenbosch university, South Africa. American Journal of Physical Anthropology 160 (1), 137–147. https://doi.org/10.1002/ajpa.22951.
R Core Team (2022). The R Project for Statistical Computing. Available online at https://www.r-project.org/ (accessed 10/27/2023).
Rivera, F./Mirazón Lahr, M. (2017). New evidence suggesting a dissociated etiology for cribra orbitalia and porotic hyperostosis. American Journal of Physical Anthropology 164 (1), 76–96. https://doi.org/10.1002/ajpa.23258.
Robinson, H. B. G./Miller, A. S./Thomas, M. E. (1983). Diseases of the teeth and supporting structures. In: R. A. Colby/H. B. G. Robinson/A. S. Miller (Eds.). Colby, Kerr and Robinson’s color atlas of oral pathology. 4th ed. Philadelphia, Lippincott, 54–56.
Rosso, P./Lederman, S. A. (1982). Nutrition in the pregnant adolescent. Current Concepts in Nutrition 11, 47–62.
Seow, W. K./Humphrys, C./Tudehope, D. I. (1987). Increased prevalence of developmental dental defects in low birth-weight, prematurely born children: a controlled study. Pediatric Dentistry 9 (3), 221–225.
South African National Department of Health (1983). Human Tissues Act 65. Government Gazette (216), 1–34.
South African National Department of Health (2004). National Policy for Health Act 61. Government Gazette (469), 66–79.
Steckel, R. H./Rose, J. C. (Eds.) (2002). The backbone of history: health and nutrition in the western hemisphere. Cambridge, Cambridge University Press.
Stinson, S. (1985). Sex differences in environmental sensitivity during growth and development. American Journal of Physical Anthropology 28 (S6), 123–147. https://doi.org/10.1002/ajpa.1330280507.
Stuart-Macadam, P. (1985). Porotic hyperostosis: representative of a childhood condition. American Journal of Physical Anthropology 66 (4), 391–398. https://doi.org/10.1002/ajpa.1330660407.
Stuart-Macadam, P. (1987). Porotic hyperostosis: new evidence to support the anemia theory. American Journal of Physical Anthropology 74 (4), 521–526. https://doi.org/10.1002/ajpa.1330740410.
Walker, P. L./Bathurst, R. R./Richman, R./Gjerdrum, T./Andrushko, V. A. (2009). The causes of porotic hyperostosis and cribra orbitalia: a reappraisal of the iron-deficiency-anemia hypothesis. American Journal of Physical Anthropology 139 (2), 109–125. https://doi.org/10.1002/ajpa.21031.
Wapler, U./Crubézy, E./Schultz, M. (2004). Is cribra orbitalia synonymous with anemia? Analysis and interpretation of cranial pathology in Sudan. American Journal of Physical Anthropology 123 (4), 333–339. https://doi.org/10.1002/ajpa.10321.
Webb, S. (1982). Cribra orbitalia: a possible sign of anaemia in pre- and post-contact crania from Australia and Papua New Guinea. Archaeology in Oceania 17 (3), 148–156. Available online at http://www.jstor.org/stable/40386604 (accessed 11/30/2023).
White, T. D./Black, M. T./Folkens, P. A. (2012). Human osteology. 3rd ed. Amsterdam, Academic Press.
Wood, J. W./Milner, G. R./Harpending, H. C./Weiss, K. M./Cohen, M. N./Eisenberg, L. E./Hutchinson, D. L./Jankauskas, R./Cesnys, G./Katzenberg, M. A./Lukacs, J. R./McGrath, J. W./Roth, E. A./Ubelaker, D. H./Wilkinson, R. G. (1992). The osteological paradox: problems of inferring prehistoric health from skeletal samples [and comments and reply]. Current Anthropology 33 (4), 343–370. https://doi.org/10.1086/204084.