BackgroundHarris Lines (HL) and Linear Enamel Hypoplasia (LEH) are non-specific skeletal markers of health status. The aetiology of these markers has not yet been confirmed due to a lack of contemporary clinical studies but is assumed to occur due to health insults associated with low socio-economic status (SES). Most studies regarding HL and LEH have been conducted on the archaeological remains of historic populations. This provides a problem when trying to determine the aetiology of the afore-mentioned defects as medical histories of those individuals being tested are unknown.
ObjectivesThis study aims to determine if there is an association between LEH and HL in a contemporary South African skeletal population with mainly low social background individuals.
Sample and MethodsThe skull and x-rays of long bones of individuals (n=592) aged between 20-90 years who lived between 1900 – 1995 sampled from the Stellenbosch University Skeletal Repository, were assessed for presence of HL and LEH.
ResultsThe study found no significant association between LEH and HL, with 7.64% of those with HL also having LEH (p=0.512). There was also no significant association between HL and LEH in females (p=0.331), but a significant association in males (p=0.027). A significant association between LEH, HL and different age-at-death groups was found in the middle group (40-59 years-of-age-at-death; p=0.006), with the least significant association in the oldest age-at-death group (>60 years-of-age-at-death; p=0.418).
ConclusionIn this South African cohort, no clear association between LEH and HL could be established, indicating that the aetiology of these disease markings should still be investigated.
Keywords: Linear enamel hypoplasia, Harris lines, Stellenbosch University Skeletal Repository, childhood physiological stress
Conflicts of interest: There are no conflicts of interest.
Citation: de Lange, J. et al. (2023). Signs of childhood physiological stresses in a South African human skeletal collection. Human Biology and Public Health 2. https://doi.org/10.52905/hbph2023.2.66.
Copyright: This is an open access article distributed under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Harris lines and linear enamel hypoplasia are non-specific markers of health status which (could be) crude markers of childhood physiological well-being. The aetiology (and pathogenesis) of these markers has not yet been confirmed due to a lack of contemporary clinical studies as most studies regarding HL and LEH have been conducted on archaeological remains of historic populations. This poses a problem when it comes to identifying the aetiology of the afore-mentioned defects.
Contents
Introduction
Non-specific markers of health status such as Harris Lines (HL) and Linear Enamel Hypoplasia (LEH) are crude markers of childhood physiological well-being, which have been studied since the 1900s and may provide insight into an individual’s medical background (Harris 1926). Harris’ lines are thin, radiopaque, sclerotic, transverse lines which develop in the metaphyses of long bones and are visible on anteroposterior radiographs (Harris 1933). Several authors have suggested that these lines form during the recovery phase after episodes of childhood diseases when longitudinal growth in bone was temporarily arrested (Aufderheide and Rodriquez-Martin 2011; Byers 1991; Larsen 2003; Park and Richter 1953; Park 1964; Platt and Stewart 1962). According to Witzel (2009), depressing effects of diseases and insufficient nutrition on the proliferation of cartilage cells in the growth plate cause the formation of these radio-dense, transverse lines. Harris’ lines form in the growing epiphyseal growth plates before their final closure. Intermediate growth arrest is characterized by the deposition of a layer of osseous tissue against the growth plate, forming horizontal trabeculae (Witzel 2009). Lines of growth arrest appear as horizontal stripes in the x-ray picture before new bone is formed at the growth plate and normal growth rates resume (Witzel 2009). It was observed that these lines decrease in frequency with age (Harris 1933; Boucherie et al. 2017). As an individual grows, the lines can undergo resorption and appear broken and thinner or even disappear with age (Boucherie et al. 2017; Caffey 1978; Garn et al. 1968). Therefore, the radiographic appearance of HL decreases with age due to bone remodelling (Marshall and Brothwell 1968). From this it can be deduced that the older an individual is and the more bone remodeling has occurred, the greater the likelihood that HL will no longer be visible. This, however, assumes that an individual is healthy and there are no factors that limit the remodelling process. Some of these markings persist into adulthood and therefore there are several factors which affect the propensity of bone to undergo resorption and remodelling including nutrition, hormonal influences, hereditary, physical activity and mechanical stress (Nakamura et al. 2018; Weber 2016).
During tooth development, enamel hypoplastic defects can occur as a result of episodic systemic disturbances during infancy and childhood, and, in contrast to bone, enamel never remodels after this formation, thus physiological stressors experienced during childhood remain permanently engraved on teeth (O’Donnell and Moes 2021). Linear enamel hypoplasia is a nonspecific quantitative enamel defect, presenting in the tooth crown enamel as a result of defects in ameloblastic activity. This dental defect represents a short period when growth slowed down or stopped during the formation of the tooth crown until the age of eruption of the last tooth (Goodman and Rose 1990; O’Donnell and Moes 2021; Steckel 2005), and the development of enamel hypoplasia is only possible during tooth crown enamel formation (Dąbrowski et al. 2021). These lines or pits are excellent measures of childhood nutritional and morbidity stress, indicating the individual’s health or/and nutritional stress during the growth stages of the first years (Goodman and Armelagos 1988; Huss-Ashmore et al. 1982). The aetiology of these markers has not yet been confirmed due to a lack of recent clinical studies, but one of the assumptions for occurrence is due to health insults associated with low socio-economic status (SES), such as malnutrition or disease (Dąbrowski et al. 2021; Gindhardt 1969; Miszkiewicz 2015; Resnick et al. 1981). Another study analysed skeletal samples (11th to 16th century) retrieved from a cemetery and priory located in Canterbury, England (Miszkiewicz 2015). According to historical studies, the socioeconomic status of those buried in the priory was higher than that of those buried in the cemetery, and those buried in the cemetery exhibited a higher prevalence and a later onset of LEH, as well as a younger age-at-death (Miszkiewicz 2015). Therefore, the lower SES of individuals impacted their overall wellbeing in a negative manner, contributing to shortened lifespans and impairments in enamel formation (Miszkiewicz 2015). These markers have also been shown to vary per population group and there is a lack of evidence regarding these insults within the South African context. In addition, these markings have been shown to occur with varying frequency in populations of different ages and can be attributed to certain factors and difficulties associated with that specific time period, such as malnutrition, localised diseases, and the introduction of antibiotics (Ameen et al. 2005; Flohr and Schultz 2009; Steyn et al. 2013).
Most studies of HL and LEH have been conducted on the archaeological remains of historic populations (Goodman et al. 1980; Goodman and Armelagos 1988; Hughes et al. 1996; McHenry 1968; Patrick 1989). This poses a problem when trying to determine the aetiology of the afore-mentioned defects as the medical history of the individuals tested is unknown, and therefore there is much speculation about the aetiologies of these defects.
The aim of the study is to determine if there is an association between LEH and HL in a South African population as represented in the Stellenbosch University Skeletal Repository in the Western Cape Province.
The hypotheses for this study are four-fold:
•
Adults that score positive for LEH also score positive for HL.
•
There is a negative correlation between HL and age-at-death due to life-long remodelling of bone that may influence the visibility of HL on the long bone shafts.
•
Sex should not show a difference in association to LEH and HL as most individuals in this repository lived in overcrowded environments, poor living conditions and little access to well-equipped hospitals or clinics during apartheid.
•
LEH and HL occurred less frequently during the early period of the 20th century when compared to later born subjects due to their shorter life span.
Sample and Methods
Sample
All materials were obtained from the Skeletal Repository Biobank (B20/04/009) housed at Stellenbosch University. The skeletons derive from the established body donation programme of the Division of Clinical Anatomy, with known age-at-death and sex information. This study was ethically cleared by the Health Research and Ethics Committee (HREC) of Stellenbosch University (S13/05/100) which conforms to the principles of the Declaration of Helsinki (World Medical Association 2013).
Individuals (n=592) in the sample were randomly selected from the list above for analysis in this study. A total of 403 individuals met the inclusion criteria for teeth, but only 349 of this cohort had LODOX® scans available to use for HL scoring.
The majority of the sample was male (70.8%; 419/592), while there was a vast under-representation of female specimens (29.2%; 173/592).
A dental inventory of each specimen in the collection was taken prior to the study and it was noted which teeth were present and scorable. Inclusion criteria for selection of the randomised sample included at least two scorable teeth on either the mandible or maxilla and that more than 50% of the tooth crown was visible. It was noted if the scorable teeth were single-rooted or multi-rooted teeth as it has been reported that canines and incisors are more sensitive to disruptive stimuli in developing teeth (Dąbrowski et al. 2021) and the grooves on molar teeth may have developed differently from the anterior or canine teeth (Reid and Dean 2006). Teeth were deemed un-scorable when calculus, severe attrition, and dental enamel defects such as caries obscured the surface of the teeth.
According to various authors, Harris’ lines are most commonly visible on both ends of the tibia, followed by the femur and the distal radius (Clarke 1980; Goodman and Armelagos 1988; Hughes et al. 1996; Maat 1984). However, a previous study of long bones from this specific population in the Western Cape (Alblas 2019) found that the tibia was most commonly affected by HL (65%), followed by the fibula (15.8%). Therefore, an inventory of tibiae and fibulae of the collection was taken prior to the study. When long bones were absent or when obstruction within the shaft of the bone due to callus formation or surgical intervention did not allow for accurate examination of the presence of HL, bones were marked as un-scorable. The criteria for evaluating HL also include having a Low dosage X-ray (LODOX® Statscan®) scan of at least one of the lower limbs (tibia or fibula).
Methods
Macroscopic visualisation of LEH was done using a ring light at 10x magnification and a dental probe was run across the tooth surface to detect grooves. The buccal and labial surfaces of the crowns of all teeth were examined according to the recommendations of Goodman and Rose (1990), as these surfaces are most frequently affected. Teeth were scored according to the presence or absence of linear grooves per tooth, the number of LEH per tooth was not taken into account.
Examination of HL was performed on each of the tibiae and fibulae present on DICOM (Digital Imaging and Communications in Medicine) radiographs taken with the LODOX® digital imaging system. An adaptation of the scoring system developed by Clark (Clark 1978) was used to determine the minimum threshold for a radiopaque transverse line to be considered a HL. The criterion for identifying HL in this study was the presence of one or more lines observable on enlarged digital LODOX® scan images in an anteroposterior position. These lines extended across the endosteal border towards the diaphysis of the tibiae and fibulae as described by Clark (1978). The lines were only scored as present if they were symmetrical on both long bones. Radiopaque lines crossing more than at least halfway across the bone were marked as having HL. The number of lines per long bone was not considered in this study, only the presence of HL and the long bone involved.
Statistics
All statistical analysis were conducted by using computer software, namely R-Studio (R Core Team 2022), as well as IBM SPSS® (2021).
First, the distribution of age-at-death was determined and subsequently grouped into three classes, namely young-adult (20-39 years-of-age-at-death), middle-adult (40-59 years-of-age-at-death) and old-adult (>60 years-of-age-at-death). The numerical value of the different ages-at-death was also considered when conducting the statistical tests (Martin 1925). The Skeletal Repository material used in this study represented individuals that lived during the 20th century (between 1900 and 1999). The 20th century was divided into three time periods, which denoted the period in which each study participant had lived. A median lifespan was then calculated. For example, an individual born in 1935 who died in 1990 lived for 55 years and reached the median lifespan in 1962.
The (1) early 20th century period (n=65) comprised individuals who reached the median lifespan between 1928 and 1940 (coinciding with economic restraints due to the Great Depression, and the pre-antibiotic period); the 2) mid-20th century period (n=260) comprised individuals who reached the median lifespan between 1941 and 1956 (a period with many socio-economic challenges, such as World War II and the start of Apartheid in South Africa, but also the introduction of antibiotics); and (3) the late 20th century period (n=267) comprised individuals who reached the median lifespan between 1957 and 1995 (representing the height of apartheid, the start of HIV infections, political unrest, and the establishment of democracy in South Africa). A St Nicolas House Analysis (SNHA) (Hermanussen et al. 2021) was conducted to obtain an overview of the correlation of the different variables of this dataset. SNHA is a statistical approach for detecting and visualizing extensive interactions among variables. The analysis provides an initial approach for clarifying potential associations that may be subject to subsequent hypothesis testing (Hermanussen et al. 2021).
A Shapiro-Wilk test (Shappiro and Wilk 1965) was performed to test normality of the distribution of the dataset. Ages-at-death were not normally distributed. Because of the non-normal distribution, Wilcoxon rank sum tests (Haynes 2013) were performed to test the hypotheses.
Pearson’s Chi-squared tests were used to assess several associations to determine if an association existed between the sex, age-at-death group or time period within the 20th century) and an association between the presence of either HL or LEH. Secondly, the test was used to evaluate if an association existed between the presence of HL and the presence of LEH per individual. Finally, the test was used to determine if the association between HL and LEH persisted through all age-at-death groups (1-3) and the time periods within the 20th century. For all statistical tests performed, (alpha) p-values <0.1 and threshold 0.0001 were considered statistically significant.
Fisher’s exact test (Sprent 2011) was performed to evaluate the association between LEH and different time periods within the 20th century, followed by the determination of the effect factor (Cohen’s W).
Data were illustrated by means of boxplots (numerical versus categorical data) and mosaicplots (categorical versus categorical data).
Results
Sample Demographics
The sample included 419 males and 173 females with an uneven ratio of 2.4:1. The ages-at-death of the sample were not normally distributed (Figure 1), as shown by the Shapiro-Wilk test for normality (W=0.99; p=0.002). The youngest known age-at-death in the present study was 20 years, and the oldest 90 years, with a mean age-at-death of 48.96 years for both males and females.
Figure 1 Distribution histogram of sample age-at-death of which the data are not normal distributed (Shapiro-Wilk normality test, W=0.99; p=0.002).
Table 1 Prevalence of LEH presence and absence based on sex
LEH absent
LEH present
total
F
count
108
12
120
prevalence
90%
10%*
100%
M
count
257
26
283
prevalence
90.8%
9.2%*
100%
total
count
365
38
403
prevalence
90.6%
9.4%
100%
* p=0.95, therefore a non-significant association
The average age-at-death of the individuals with LEH in this study was 40.2 years (range: 21-81 years). The young-adult age-at-death group demonstrated a higher frequency of LEH than the other two age-at-death groups [4.71% (young-adult group) vs. 3.47% (middle-adult group) and 1.24% (old-adult group); p<0.01]. The late time period showed a slightly significant increase in the frequency of LEH when compared to the other two time periods (7.20% (late) vs. 0.25% (early) and 1.99% (mid); p=0.02) (Figure 2).
Figure 2 Mosaicplot of LEH frequency in the three different time periods of the 20th century (1=early; 2=mid; 3=late; LEH: 1=No lines present across teeth; 2=Lines present across teeth).
There was a significant association between the prevalence of LEH and the age-at-death (Wilcoxon rank sum test, p=0.0002) with an effect factor of 0.61 (Cohen’s D), but no association between sex and LEH (Pearson’s Chi-squared test, p=0.950). Figure 3 shows the prevalence of LEH and HL in the different age-at-death groups.
Figure 3 Distribution box (median, 25th and 75th centile) and whiskers (range) of LEH (left) and HL (right) prevalence in different age-at-death groups (1=No lines present across teeth; 2=Lines present across teeth).
All available digital LODOX® images 349/592 (59%) were examined for HL. HL were present in the tibiae and fibulae of 144 (41.26%) individuals. The average age-at-death of individuals with HL was 48.9 years (range: 22-82 years, SD: 13.2 years). There was no age-at-death difference in individuals with and without HL (Wilcoxon rank sum test, p= 0.687; Figure 3).
Pearson’s Chi-squared test revealed a non-significant relationship between sex and HL (p=0.340). There was also no significant association between the time period of the 20th century and the presence of HL (Pearson’s Chi-Squared test, p-value of 0.839).
Eleven of 114 individuals (7.64%) with HL also showed LEH, but the association between the presence of HL and LEH was not significant (Spearman Chi-squared test, p=0.512, Table 2).
Table 2 The percentage of individuals with and without HL and LEH. Highlighted percentages represent those with both HL and LEH
LEH absent
LEH present
total
HL absent
count
114
19
133
prevalence
85.7%
14.3%
100%
HL present
count
93
11
104
prevalence
89.4%
10.6%*
100%
total
count
207
30
237
prevalence
87.3%
12.7%
100%
* p=0.512, not significant
The combination of both LEH and LH was more frequent in females (p=0.042, Table 3). The association between HL and LEH was only significant in males (p=0.027), but not in females (p=0.331).
Table 3 Association between HL and LEH based on sex (p=0.042)
LEH absent
LEH present
total
F
HL absent
count
36
4
40
prevalence
90%
10%
100%
HL present
count
28
6
34
prevalence
82.4%
17.7%*
100%
total
count
64
10
74
prevalence
86.5%
13.5%
100%
M
HL absent
count
78
15
93
prevalence
83.9%
16.1%
100%
HL present
count
65
5
70
prevalence
92.9%
7.1% **
100%
total
count
143
20
163
prevalence
87.7%
12.3%
100%
*p=0.331; **p=0.027
The combination of both HL and LEH with age-at-death was significant (Wilcox test, p=0.0002, Figure 4) and particularly frequent at younger age-at-death. The association between HL and LEH was only significant in the middle age group (40-59 years-at-death; Spearman Chi-squared test, p=0.006, Table 4).
Figure 4 Distribution box (median, 25th and 75th percentile) and whiskers (range) of HL versus LEH prevalence at different ages-at-death (1:1=No lines present across bones or teeth; 2:1=Lines present across bones, but no lines present on teeth; 1:2=No lines present on bones, but lines present across teeth; 2:2= Lines present on bones and teeth).
Table 4 Association between HL and LEH in different age-at-death groups
LEH absent
LEH present
total
Y
HL absent
count
31
6
37
prevalence
83.8%
16.2%
100%
HL present
count
20
8
28
prevalence
71.4%
28.6%
100%
total
count
51
14
65
prevalence
78.5%
21.5%
100%
A
HL absent
count
62
11
73
prevalence
84.9%
15.1%
100%
HL present
count
54
2
56
prevalence
96.4%
3.6% *
100%
total
count
116
13
129
prevalence
89.9%
10.1%
100%
O
HL absent
count
21
2
23
prevalence
91.3%
8.7%
100%
HL present
count
19
1
20
prevalence
95%
5%
100%
total
count
40
3
43
prevalence
93.0%
7.0%
100%
*p=0.006
Lastly, a Spearman Chi-squared test was used to assess the relationship between the different time periods within the 20th century and the association between HL and LEH. It was found that there was a significant association in only the mid (p=0.009) and late time period within the 20th century (p=0.038), with the least significant association recorded in the early time period within the 20th century (p=0.242).
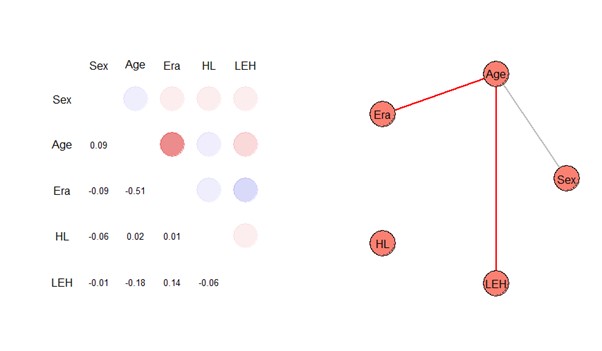
Figure 5 shows the correlation matrix of all variables. A St. Nicolas House Analysis (SNHA) illustrates significant chains of associations between these variables and again highlights the independent position of HL among the other variables.
Figure 5 St Nicolas House Analysis where blue colour circles indicate positive, and red colour circles indicate negative correlations (HL= Harris Lines; LEH= Linear Enamel Hypoplasia; Era = time period in the 20th century).
Discussion
Harris Lines (HL) and Linear Enamel Hypoplasia (LEH) are non-specific skeletal markers of health status. The aim of this study was to determine if there is an association between LEH and HL in a South African population as represented in the Stellenbosch University Skeletal Repository. Many of the finding of this study are in accordance with previous findings (Caffey 1978; Clarke 1980; Mays 1995; Webb 1984).
LEH
Within the current study, the prevalence of LEH was 9.43%, which falls within the variety of prevalence’s found by previous authors which range from 3% to 99% (Pascoe and Seow 1994; Seow et al. 1987)
A Wilcoxon rank sum test revealed a significant relationship between age-at-death and LEH where the young age groups show the greatest prevalence of LEH. This is in accordance with Ribot and Roberts (1996), who found that the greatest prevalence of LEH occurred between nine to fifteen years-of-age. However, it is an unexpected finding due to the nature of teeth and the processes by which they form. Unlike bone, remodelling does not take place in the dentition and therefore once the defect is present on the enamel surface, it will remain visible for the remainder of the individual’s life unless the crown surface itself becomes damaged (Hillson and Bond 1997). A reason for the higher prevalence in younger age groups may be the developmental timing of tooth formation and the cumulative effect of enamel disruptions over time. Another possible explanation for this finding could simply be that the individuals in this study sample, who formed LEH, were frailer than those who did not form LEH. This is supported in the context of the osteological paradox limitations as described by Wood et al. (1992). The limitations and complexities involved in using skeletal remains should be taken into account and should allow for the underlying vulnerabilities in the skeletal population. O’Donnell and Moes (2021) mentioned a few studies showing that LEH may also be associated with higher mortality risks and earlier deaths, likely from its correlation with factors associated with mortality, such as socioeconomic standing. Furthermore, Ham et al. (2021) examined the impact of LEH on survival in the Pueblo Bonito community (Chaco Canyon) and the Hawikku community (Zuni). Their results indicated that, compared to individuals without LEH, those with LEH had a shorter mean survival time (Ham et al. 2021).
Persons who reached their median lifespan late in the 20th century in the time period between 1957 and 1995 showed the highest frequency of LEH (p=0.020), suggesting a decrease in dental health over the 20th century as environmental and social conditions deteriorated due to apartheid law influences on the populations. However, it has been noticed that dental work became more prevalent in the late time period, since the dentist to population ratio gradually improved towards the late 20th century (Rensburg and Mans 1990). There was no sex difference in the deterioration of dental health as already observed in a Polish sample studied by Kozak and Krenz-Niedbala (2002), as well as a study conducted by Infante and Gillespie (1974). Kozak and Krenz-Niebdala (2002) analysed the frequency of cribra orbitalia by sex and age-at-death and its association with enamel hypoplasia in a medieval population from northern Poland. They observed no clear relation between the lesion and sex, and no association of cribra orbitalia and enamel hypoplasia (Kozak and Krenz-Niedbala 2002).
HL
A higher average age-at-death was observed in individuals with HL in comparison with those having LEH, with no significant difference between the age-at-death of individuals with or without HL. This is in contrast with the findings of Harris (1933), who observed that these lines decrease in frequency with age as well as Marshall and Brothwell (1968), who stated that the radiographic appearance of HL will decrease with age due to remodelling of bone. We therefore reject our second hypothesis as we were unable to find a negative correlation between LH and age-at-death.
We noted a small, but insignificant sex difference in the prevalence of HL with more HL in males (67.4%) than in females (32.6%). This finding is in accordance with other authors (Ameen et al. 2005; Huss-Ashmore et al. 1982; Webb 1984), who have also noted no significant difference between the sexes’ prevalence to develop HL.
The prevalence of HL did not show a significant difference between the three time periods of the 20th century. Weak correlations with the early time period for growth arrest lines were observed, with a stronger correlation in the mid- and late time period.
Before the advance of antibiotics, localised infections, such as periostitis and osteomyelitis seen on bone, and associated complications had a severe impact on the daily lives of individuals (Flohr and Schultz 2009), often resulting in death, thereby potentially explaining the low HL frequency in the Skeletal Repository sample during this time period. After the introduction of antibiotics in the 1940s, infections were treated successfully, resulting in a longer life span, but also chronic diseases as result of recurring infections (Steyn et al. 2013). Such chronic infections can result in permanent osseous changes in the bones (Flohr and Schultz 2009), explaining the increase in HL seen in the mid- and late 20th century. However, it should also be taken in consideration that the early period is under-represented in the Skeletal Repository sample compared to the mid- and late 20th century periods.
LEH vs. HL
The current study did not find a significant association between HL and LEH, as previously noted in various studies (Böker et al. 2022; Caffey 1978; Webb 1984) and thus failed to support our first hypothesis that adults that score positive for LEH also score positive for HL. Böker et al. (Böker et al. 2022) also found dental eruption to be an independent biological maturation system that is regulated by mechanisms different than those of skeletal age and height. Although Maat (Maat 1984) proposed that a correlation between these two defects would exist due to their presumably shared aetiology, several authors have discredited this claim (Caffey 1978; Clarke 1980; Webb 1984; Mays 1995). More recently, a study conducted on an archaeological sample from Chile took into account the time of formation of both HL and LEH and found that HL showed greatest prevalence during an individual’s first year of life as well as during adolescence, whereas the greatest prevalence noted for LEH clustered around three to five years-of-age (Alfonso et al. 2005). There may thus be an explanation for the lack of correlation between HL and bone remodelling in the first few years of life. Compared with bone growth, dental development appears to be much less affected by environmental stress (Papageorgopoulou et al. 2011). HL can, therefore, consequently be associated with trivial stress episodes, but not LEH (Papageorgopoulou et al. 2011). It was therefore hypothesised that HL may occur as a result of normal saltatory growth due to an individual’s rapid bone formation during times of growth spurts (Alfonso et al. 2005; Papageorgopoulou et al. 2011). In contrast, some overlap has been noted regarding the time of formation of these defects and therefore, it cannot be said with surety that there is no association (Meurs 2014).
A significant correlation between sex and the association between LEH and HL was found in males (p=0.027). This finding is in contrast with a study conducted by Alfonso et al. (2005), who found no significant association between sex, LEH and HL. A difference in frequency of LEH and HL in sexes were not expected as both sexes in this skeletal population were exposed to unsanitary conditions associated with poor housing and overcrowding environments, and less success in buffering themselves from malnutrition and exposure to pathogens. Thus, we partially rejected our third hypothesis that sex was not associated with the occurrence of LEH and HL.
There was also a higher prevalence of individuals that presented with both LEH and HL in the younger age-at-death group, in comparison to the other two groups. This can potentially be attributed to the small sample size in the young aged group and individuals that presented with both LEH and HL in this group.
A significant correlation was found between the mid- and late 20th-century periods and the association between LEH and HL. This finding can be attributed to the high prevalence of both LEH and HL during those time periods, as reported previously. The skeletons from the late period of the study, which corresponds to the apartheid era characterized by poor living conditions, political unrest, and pathogen exposure, showed the consequences of this regime. From the 1960s onwards, LEH and HL became more prevalent compared to earlier times.
This study was considered in the context of the osteological paradox limitations first described by Wood et al.(1992) when interpreting LEH and HL lesions as indicators of health in this skeletal population. Understanding the survivorship bias inherent in skeletal collections allows researchers to acknowledge that the individuals represented in the sample have already surpassed a certain threshold of survival, indicating that they were resilient enough to reach adulthood despite the challenging living conditions. This recognition helps contextualize the presence of LEH as a marker of stress or disruption during tooth development. By considering the socioeconomic factors and potential hardships faced by the population, researchers can infer that the prevalence and severity of LEH likely reflect the overall burden of nutritional deficiencies, illness, and other stressors experienced within the community. Consequently, the osteological paradox provides a framework for interpreting LEH as an indicator of the population's health challenges and can contribute to a more nuanced understanding of their socioenvironmental circumstances.
Conclusion
In accordance with previous findings, a statistically significant association between HL in the lower limbs of individuals and LEH on available teeth was not noted, but a significant positive correlation was, however, found between sex and the association between LEH and HL in males. It was also found that this association decreased with age, and, additionally, a significant positive correlation was identified between the mid- and late time periods within the 20th century and the association between LEH and HL.
Overall, the aim of the present study was met, many known factors regarding HL and LEH have been confirmed and additional findings have been highlighted. LEH and HL were found not to be significantly correlated in the current study. In line with previous findings, this study concludes that dental eruptions are not regulated by the same mechanisms as those determining skeletal age or height, which are independent, biological maturation systems. No correlation was found between sex and the association between LEH and HL and remodelling could be observed over time (age). In addition, a significant association between LEH, HL and different age-at-death groups was found in the 40-59 years-of-age-at-death group. However, much is still unknown about these defects and an abundance of additional research should be conducted to obtain a full understanding of these defects. Since HL did not show a statistically significant association to LEH, it is imperative to re-examine HL as purely nutritional or pathological stress markers.
Acknowledgements
This manuscript and statistical analysis were the result of the participation in the 5th International Summer School in Gülpe, Brandenburg, Germany from 18th to 24th of July 2022. Special thank you to PD Dr Christiane Scheffler, Dr Detlef Groth, Prof Michael Hermanussen and Prof Barry Bogin for sponsoring the week as well as their patient assistance during the summer school. The authors express their gratitude towards the University of Potsdam and KoUp for funding the travel costs to attend the International Summer School. The authors would also like to thank the anonymous donors for the selfless donation of their bodies for use in our skeletal analysis.
References
Alblas, M. (2019). Assessment of health status in a 20 th century skeletal collection from the Western Cape. Available online at https://www.academia.edu/70366163 (accessed 6/5/2023).
Alfonso, M. P./Thompson, J. L./Standen, V. G. (2005). Reevaluating Harris lines‐a comparison between Harris lines and enamel hypoplasia. Collegium antropologicum 29 (2), 393–408.
Ameen, S./Staub, L./Ulrich, S./Vock, P./Ballmer, F./Anderson, S. E. (2005). Harris lines of the tibia across centuries: a comparison of two populations, medieval and contemporary in Central Europe. Skeletal radiology 34 (5), 279–284. https://doi.org/10.1007/s00256-004-0841-3.
Aufderheide, A. C./Rodriquez-Martin, C. (2011). The Cambridge encyclopedia of human paleopathology. Cambridge University Press.
Böker, S./Hermanussen, M./Scheffler, C. (2022). Dental age is an independent marker of biological age. Human Biology and Public Health 3. https://doi.org/10.52905/hbph2021.3.24.
Boucherie, A./Castex, D./Polet, C./Kacki, S. (2017). Normal growth, altered growth? Study of the relationship between harris lines and bone form within a post-medieval plague cemetery (Dendermonde, Belgium, 16th Century). American Journal of Human Biology 29 (1). https://doi.org/10.1002/ajhb.22885.
Byers, S. (1991). Calculation of age at formation of radiopaque transverse lines. American Journal of Physical Anthropology 85 (3), 339–343. https://doi.org/10.1002/ajpa.1330850314.
Clark, S. (1978). Markers of metabolic insult: the association of radiopaque transverse lines, enamel hypoplasias and enamel histopathologies in a prehistoric human skeletal sample. Ph.D.Dissertation. University of Colorado, Boulder.
Clarke, S. (1980). Early childhood morbidity trends in prehistoric populations. Human Biology 52 (1), 79–85.
Dąbrowski, P./Kulus, M. J./Furmanek, M./Paulsen, F./Grzelak, J./Domagała, Z. (2021). Estimation of age at onset of linear enamel hypoplasia. New calculation tool, description and comparison of current methods. Journal of Anatomy 239 (4), 920–931. https://doi.org/10.1111/joa.13462.
Flohr, s./Schultz, M. (2009). Osseous changes due to mastoiditis in human skeletal remains. International Journal of Osteoarchaeology 19 (1), 99–106. https://doi.org/10.1002/oa.961.
Garn, S. M./Silverman, F. N./Hertzog, K. P./Rohmann, C. G. (1968). Lines and bands of increased density. Their implication to growth and development. Medical radiography and photography 44 (3), 58–89.
Gindhardt, S. (1969). The frequency of appearence of transverse lines in the tibia in relation to childhood illnesses. American Journal of Physical Anthropology 31 (1), 17–22.
Goodman, A. H./Armelagos, G. J. (1988). Childhood stress and decreased longevity in a prehistoric population. American Anthropologist 90 (4), 936–944. https://doi.org/10.1525/aa.1988.90.4.02a00120.
Goodman, A. H./Armelagos, G. J./Rose, J. C. (1980). Enamel hypoplasias as indicators of stress in three prehistoric populations from Illinois. Human Biology 52 (3), 515–528.
Goodman, A. H./Rose, J. C. (1990). Assessment of systemic physiological perturbations from dental enamel hypoplasias and associated histological structures. American Journal of Physical Anthropology 33 (S11), 59–110. https://doi.org/10.1002/ajpa.1330330506.
Ham, A. C./Temple, D. H./Klaus, H. D./Hunt, D. R. (2021). Evaluating life history trade-offs through the presence of linear enamel hypoplasia at Pueblo Bonito and Hawikku: a biocultural study of early life stress and survival in the Ancestral Pueblo Southwest. American Journal of Human Biology 33 (2). https://doi.org/10.1002/ajhb.23506.
Harris, H. A. (1933). Bone growth in health and disease. The biological principles underlying the clinical, radiological, and histological diagnosis of perversions of growth and disease in the skeleton. Oxford University Press.
Haynes, W. (2013). Wilcoxon Rank Sum Test. In: Werner Dubitzky/Olaf Wolkenhauer/Kwang-Hyun Cho et al. (Eds.). Encyclopedia of Systems Biology. New York, NY, Springer New York, 2354–2355.
Hermanussen, M./Aßmann, C./Groth, D. (2021). Chain reversion for detecting associations in interacting variables—St. Nicolas House Analysis. International Journal of Environmental Research and Public Health 18 (4), 1741. https://doi.org/10.3390/ijerph18041741.
Infante, P. F./Gillespie, G. M. (1974). An epidemiologic study of linear enamel hypoplasia of deciduous anterior teeth in Guatemalan children. Archives of Oral Biology 19 (11), 1055–1061. https://doi.org/10.1016/0003-9969(74)90095-8.
Kozak, J./Krenz-Niedbala, M. (2002). The occurrence of cribra orbitalia and its association with enamel hypoplasia in a medieval population form Kolobrzeg, Poland. Variability and Evolution 10 (1), 75–82.
Larsen, C. S. (2003). Bioarchaeology. Interpreting behavior from the human skeleton. Cambridge, Cambridge Univ. Press.
Maat, G. J. R. (1984). Dating and rating of Harris’s lines. American Journal of Physical Anthropology 63 (3), 291–299. https://doi.org/10.1002/ajpa.1330630305.
Marshall, W./Brothwell, D. (1968). Problems in relating the presence of transverse lines in the radius to the occurrence of disease. The skeletal biology of earlier human populations.
Mays, S. (1995). The relationship between Harris Lines and other aspects of skeletal development in adults and juveniles. Journal of Archaeological Science 22 (4), 511–520. https://doi.org/10.1006/jasc.1995.0049.
McHenry, H. (1968). Transverse lines in long bones of prehistoric California Indians. American Journal of Physical Anthropology 29 (1), 1–17. https://doi.org/10.1002/ajpa.1330290110.
Meurs, M. (2014). A matter of lines, a study of Harris lines and enamel hypoplasia in the late medieval collection of Paardenmarkt, Alkmaar. Leiden, Leiden University. Available online at https://hdl.handle.net/1887/23178 (accessed 5/5/2023).
Miszkiewicz, J. J. (2015). Linear enamel hypoplasia and age-at-death at medieval (11 th -16 th centuries) St. Gregory’s priory and cemetery, Canterbury, UK. International Journal of Osteoarchaeology 25 (1), 79–87. https://doi.org/10.1002/oa.2265.
Nakamura, N./Rodeo, S./Alini, M./Maher, S./Madry, H./Erggelet, C. (2018). Physiology and pathophysiology of musculoskeletal tissues. 4th ed. Elsevier Inc.
O’Donnell, L./Moes, E. (2021). Sex differences in linear enamel hypoplasia prevalence and frailty in ancestral Puebloans. Journal of Archaeological Science: Reports 39, 103153. https://doi.org/10.1016/j.jasrep.2021.103153.
Papageorgopoulou, C./Suter, S. K./Rühli, F. J./Siegmund, F. (2011). Harris lines revisited: prevalence, comorbidities, and possible etiologies. American Journal of Human Biology 23 (3), 381–391. https://doi.org/10.1002/ajhb.21155.
Park, E. A. (1964). The imprinting of nutritional disturbances on the growing bone. Pediatrics 33, SUPPL:815-862.
Park, E. A./Richter, C. P. (1953). Transverse lines in bone: the mechanism of their development. Bulletin of the Johns Hopkins Hospital 93, 234–248.
Pascoe, L./Seow, W. K. (1994). Enamel hypoplasia and dental caries in Australian aboriginal children: prevalence and correlation between the two diseases. Pediatric dentistry 16 (3), 193–199.
Patrick, M. K. (1989). An archaeologiocal, anthropological study of the human skeletal remains from the Oakhurst Rockshelter, George, Cape Province, Southern Africa. University of Cape Town.
Platt, B. S./Stewart, R. J. (1962). Transverse trabeculae and osteoporosis in bones in experimental protein-calorie deficiency. The British journal of nutrition 16, 483–495.
R Core Team (2022). The R Project for Statistical Computing. Available online at https://www.r-project.org/ (accessed 10/27/2023).
Rensburg, H. C. J. van/Mans, A. (1990). Profile of disease and health care in South Africa. 2nd ed. Pretoria, Academia.
Resnick, Donald/Draud, Lee Ann/Fix, Catherine F./Trudell, Debra J./Holbrook, Michael R./Velligan, Joyce (Eds.) (1981). Diagnosis of bone and joint disorders. Philadelphia, W. B. Saunders Company.
Ribot, I./Roberts, C. (1996). A study of non-specific stress indicators and skeletal growth in two mediaeval subadult populations. Journal of Archaeological Science 23 (1), 67–79. https://doi.org/10.1006/jasc.1996.0006.
Seow, W. K./Humphrys, C./Tudehope, D. I. (1987). Increased prevalence of developmental dental defects in low birth-weight, prematurely born children: a controlled study. Pediatric dentistry 9 (3), 221–225.
Shappiro, S. S./Wilk, M. B. (1965). An analysis of variance test for normality (complete samples). Biometrika 52 (3-4), 591–611.
Sprent, P. (2011). Fisher Exact Test. In: Miodrag Lovric (Ed.). International Encyclopedia of Statistical Science. Berlin, Heidelberg, Springer Berlin Heidelberg, 524–525.
Steckel, Richard H. (Ed.) (2005). The backbone of history. Health and nutrition in the western hemisphere. Cambridge, Cambridge Univ. Press.
Steyn, M./Scholtz, Y./Botha, D./Pretorius, S. (2013). The changing face of tuberculosis: trends in tuberculosis-associated skeletal changes. Tuberculosis (Edinburgh, Scotland) 93 (4), 467–474. https://doi.org/10.1016/j.tube.2013.04.003.
Webb, S. (1984). Intensification, population and social change in south-eastern Australia: the skeletal evidence. Aboriginal History Journal 8, 154–172. https://doi.org/10.22459/AH.08.2011.10.
Weber, T. J. (2016). Osteoporosis. In: L. Goldman/A. I. Schafer (Eds.). Goldman-Cecil medicine. 25th ed. Philadelphia, Pennsylvania, Elsevier Saunders, 1637-1645.e3.
Wood, J. W./Milner, G. R./Harpending, H. C./Weiss, K. M./Cohen, M. N./Eisenberg, L. E./Hutchinson, D. L./Jankauskas, R./Cesnys, G./Katzenberg, M. A./Lukacs, J. R./McGrath, J. W./Roth, E. A./Ubelaker, D. H./Wilkinson, R. G. (1992). The osteological paradox: problems of inferring prehistoric health from skeletal samples [and Comments and Reply]. Current Anthropology 33 (4), 343–370. https://doi.org/10.1086/204084.
World Medical Association (2013). Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 310 (20), 2191–2194. https://doi.org/10.1001/jama.2013.281053.
 ✉
✉