What does stunting tell us?
Christiane Scheffler ✉
✉
University of Potsdam, Human Biology, 14469 Potsdam, Germany
Michael Hermanussen
Aschauhof 3, 24340 Eckernförde – Altenhof, Germany
DOI: https://doi.org/10.52905/hbph2022.3.36
Abstract
Stunting is commonly linked with undernutrition. Yet, already after World War I, German
pediatricians questioned this link and stated that no association exists between nutrition
and height. Recent analyses within different populations of Low- and middle-income
countries with high rates of stunted children failed to support the assumption that
stunted children have a low BMI and skinfold sickness as signs of severe caloric
deficiency. So, stunting is not a synonym of malnutrition. Parental education level has a
positive influence on body height in stunted populations, e.g., in India and in Indonesia.
Socially disadvantaged children tend to be shorter and lighter than children from affluent
families.
Humans are social mammals; they regulate growth similar to other social mammals. Also in
humans, body height is strongly associated with the position within the social hierarchy,
reflecting the personal and group-specific social, economic, political, and emotional
environment. These non-nutritional impact factors on growth are summarized by the concept
of SEPE (Social-Economic-Political-Emotional) factors. SEPE reflects on prestige,
dominance-subordination, social identity, and ego motivation of individuals and social
groups.
Keywords: malnutrition, SEPE factors, physical fitness, height in history
Conflicts of interest: There are
no conflicts of interest.
Citation: Scheffler, C. / Hermanussen, M. (2022). What does stunting tell us?. Human Biology and Public Health 3. https://doi.org/10.52905/hbph2022.3.36.
Copyright: This is an open access article distributed under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22-05-2022 | Accepted: 12-12-2022 | Published: 10-03-2023
Take-home message for students
Stunting is not a synonym of under- or malnutrition. The regulation of body height is
closely related to social, economic, political, and emotional factors. Being shorter than
average may, thus, reflect shortcomings in any of these factors and/or poor parental
education. Stunting in the modern sense has been the natural condition of human height for
more than 10.000 years.
Contents
Stunting – the common knowledge
WHO-UNICEF reports that globally 144 million children (21.3%) under 5 years were stunted in
2019 (WHO 2021).
Stunting is defined as low height-for-age. “Stunting” means “short” – nothing else. It is
considered the result of chronic or recurrent undernutrition, usually associated with
poverty, poor maternal health and nutrition, frequent illness, and/or inappropriate feeding
and care in early life (WHO 2022).
The term stunting is commonly linked with undernutrition. More than 23.700 publications are
listed in pubmed under the keywords “stunting+malnutrition+undernutrition”, documenting the
common interpretation of stunting as being associated with nutrition. Meanwhile the terms
“stunting”, “malnutrition”, and “undernutrition” are used as synonyms in the
epidemiological, medical, and scientific literature. Prendergast and Humphrey (2014) have summarized: “Linear growth failure is the
most common form of undernutrition globally”.
Lartey states that “there is convergence among the nutrition community on the use of
length-for-age as the indicator of choice in monitoring the long-term impact of chronic
nutritional deficiency” (Lartey 2015).
But is this true?
The current definition of stunting is an inappropriate mixture of (1) a statistical
statement and (2) an incomplete list of explanations. Many factors cause shortness of body
height, but short body height is not proof of these factors. The current definition of
stunting needs disentanglement, and as long as the list of explanations is considered part
of this definition, it is essential to include the full spectrum of influencing factors.
These are influences from social, economic, political, and emotional (SEPE) sources.
Nutrition is a prerequisite of growth. Lack of nutrition inhibits growth. There is ample
evidence also in historic studies that this is the case. Keys et al. (Keys et al. 1950) explicitly state that “there can be no doubt from the
evidence in the literature that the growth of children can be and is influenced by a
restriction in the food intake”. However, reversing the line of argument by connecting short
stature with shortage of food lacks substantiation (Hermanussen and Wit 2017).
Macro- and micronutrient deficits lead to a growth retardation. This is usually a
retardation in tempo (Hermanussen and Scheffler
2022). Growth retardations are usually followed by catch-up growth when the
deficits have been compensated for. In cases of long-lasting deficits children my remain
stunted. When stunding was caused by nutrition deficits nutritional intervention always have
a remarkable impact on growth. This however is not the case in most stunted populations.
Goudet et al. (2017) reviewed in a Cochrane study
15 intervention studies of macro- and micronutrients mainly located in Bangladesh, India,
and Peru and found no evidence of an effect or unclear effect of nutrient supplementation in
children. Other studies show marginal positive effects on height. Several authors found no
effect of supplementary feeding on height, height-for-age or height-for-weight values in
low- and middle-income countries (LMIC), e.g., Indonesia or Guatemala, in the various
intervention programs (Goudet et al. 2017; Griffen 2016; Kristjansson et al. 2015; Sguassero et al.
2012; Uauy et al. 2011).
But why are so many children stunted, especially in the low- and middle-income
countries?
What do we know from history?
Starvation and undernutrition have always been present in human prehistory and history and
have frequently been reported (Rosenstock et al.
2019; Dikanski 1914; Wilke et al. 2021; Scheffler and
Hermanussen 2022). Precise documents of growth and development of European children
living under various condition are available since the 19th century, though most of these
publications have little or no readership due to poor accessibility and language barriers
(Hermanussen et al. 2018).
Severe maternal starvation is associated with smaller size already at birth. Multiple
historic birth weight data support this association, including data from the siege of
Leningrad (Antonov 1947) and the Dutch famine of
1944/45 (Dutch hunger winter near the end of World War II) (Rooij et al. 2010).
Nutrition has only a distinct impact on growth during pregnancy and early childhood under
severe starvation. This is different under mild caloric restriction. Humans have evolved to
react with phenotypic plasticity – not only but also in growth – to a broad frame of
environmental conditions, including variation in nutrition. Nutrition has always been a
limiting factor, and growth patterns of children are adapted to react. If a mother is
suffering from mild starvation during pregnancy, the fetus and later a breastfed child will
still get enough food to grow. Compensation mechanisms exist. In the case of mild
malnutrition, intrauterine countermeasures are taken and the affected fetus even grows
better – this was stated by Antonov (1947), and a
similar statement had already been made by Gassner (1862). Mildly undernourished mothers tend to increase their investment of energy
in the actual offspring as a biological answer of the life history tradeoff between actual
and future offspring. If the mother had stored her energetic reserves for future offspring,
the current offspring would have been left with a lower chance of survival.
This is different in children older than 2 years and in adolescents. Already at the end of
the 19th century and in view of the catastrophic nutritional situation of the German
civilian population suffering from mass starvation particularly in the winter 1916/17 near
the end of World War I and shortly thereafter, German pediatricians had observed that even
severely undernourished children and adolescents completely caught up in height growth, and
explicitly stated that “the longitudinal growth of the child is largely independent of the
extent and type of nutrition...” (Schlesinger
1919).
The same was observed in persons exposed to the “Dutch famine” during the winter of
1944/45. Adult women exposed to famine as children before the age of one year reached 4.45
cm less adult height, and 4.08 cm less adult height when exposed before the age of 2 years.
Adult males exposed to famine before age one are 3.16 cm shorter, and when exposed before
age 2 are 4.09 cm shorter than when exposed at an older age (Portrait et al. 2017).
It appears that the first 1000 days of life are critical for optimal growth and
development. This period is sensitive due to the rapid development, increased energy needs,
and the changing nutrient requirement (Beluska-Turkan
et al. 2019). Starvation in early childhood restricts growth and leads to shorter
body height. Yet, even when considering the 4 cm loss in adult height of the Dutch exposed
to the famine in 1944/45, these people are not stunted. At present, the average final height
is 184.0 cm for young men and 170.6 cm for young women (Fredriks et al. 2000). At this point, it may be useful to mention that the minute
effects of undernutrition on height clearly contrast the well-known detrimental effects of
prenatal and early infant undernutrition on the future regulation of body weight and
metabolism.
Based on very similar observations in German schoolchildren, Koch (1935) explicitly wrote that “food would have been quite a handsome
explanation for the increase in linear growth. But linear growth has been demonstrated to be
almost independent of this factor … Size recklessly increases even during marked
undernutrition … until the body has wasted its last depot. One might talk about parasitic
growth in length”.
Several pediatricians explicitly questioned any prominent role of nutrition and instead
highlighted the association between economic affluence, social strata, (Adriany and Tesar 2022) and growth. The German
pediatrician Meinhard von Pfaundler (1916) stated
that „this question [short stature of the socially disadvantaged children] is important when
considering the reason for the undersize of the poor. Malnutrition has often been mentioned,
but, it does not seem appropriate to me to address malnutrition as the decisive factor in
the undersize of the poor.” Pfaundler particularly emphasized that these people’s body
weight is not reduced to the extent that the reduction in body length would suggest but, in
fact, less. The differences are not great but quite constant. Other authors of the early
20th century published similar observations (Hermanussen
et al. 2018) and later also pointed to the importance of emotional deprivation and
its effect on infant and child growth (Scheffler et al.
2021a).
Severe undernutrition impairs growth and goes along with characteristic clinical signs like
edema, Bitot’s spots, goiter, and typical changes in hair, skin, and general appearance
(Behrman et al. 1999). Undernourished children are
not only short for age but also delayed in developmental tempo (Hermanussen and Scheffler 2022). A seminal Mexican study published by
Gomez et al. (1955) reported on 584 severely
malnourished children submitted to the Hospital Infantil, Mexico City, in the early 1950s.
90% of them were aged between 6 months and 5 years. Weight was “from 40 to 60 per cent of
the average normal theoretic weight in 509 children, and under 40 per cent in 75 children”.
In these children, the authors found that “the difference in height from the normal
theoretic height increases with the age of the child; at 5 years, the difference was 15.8
per cent”. This study marked the starting point of the modern debate on stunting.
Drawing on these observations, Waterlow (1972)
introduced a medical classification of malnutrition based on height-for-age that served as
the basis for the modern understanding of the causes of short stature. He presented it by
the example of “two hypothetical children”, rather than empirical data. The term “stunting”
has become a synonym for malnutrition in scientific literature since an international Nestlé
workshop in 1988 (Waterlow 1988).
The political consequences of this interpretation are severe: populations with significant
numbers of stunted children are pressured into implementing nutritional interventions even
though the effect of such interventions has been shown to be only marginally relevant for
body height and, on the contrary, boost the prevalence of child obesity (Goudet et al. 2017).
Stunting is not a synonym of malnutrition
Starvation is a severe deficiency in caloric energy intake, below the level needed to
maintain an organism's life (UIA 2022). Starvation
leads to decrease in body mass, respectively BMI, skinfold thickness, and mid upper-arm
circumference (MUAC). Therefore, these parameters have been used as indicators for caloric
undernutrition in recent populations. Based on the prevalent perception that stunting is
linked with starvation, we might hypothesize that in stunted populations strong positive
associations exist between body height and caloric intake, respectively with related
parameters like BMI, skinfold thickness, or MUAC.
However, this is not the case. Mumm and Scheffler (2019) re-analyzed data of the Young Life Study originally performed to investigate
associations between poverty and stunting in Ethiopia, Vietnam, Peru, and India. Scheffler
et al. (2018) also analyzed data from India as well
as from Indonesian schoolchildren (Scheffler et al.
2020; Scheffler et al. 2021a) and in all
cases failed to show any relevant association between body height and anthropometric
parameters related to caloric intake.
Whereas anthropometric data are often freely available, information about the individual
nutritional intake are rare. Even in careful studies such as the longitudinal study “Young
Lives – Measuring Child Poverty and Health” (Boyden
2022; Jones 2018; Woldehanna et al. 2018; Mumm and
Scheffler 2019), the information on food consumption, e.g., pasta/rice, meat, fish,
milk, vegetables/fruit, cheese, sweets, etc., is limited to information per household.
Re-analyzing household food consumption failed to show any clear pattern of food groups
related to height, neither within the same country nor between countries (Mumm and Scheffler 2019). There was no relevant
association between the amounts of nutritional intake of protein, fats, carbohydrates,
vegetables and fruit, sweets, or processed food, and body height and weight in stunted
populations. Figure 1 illustrates the lack of
association between body height and various nutritional components.
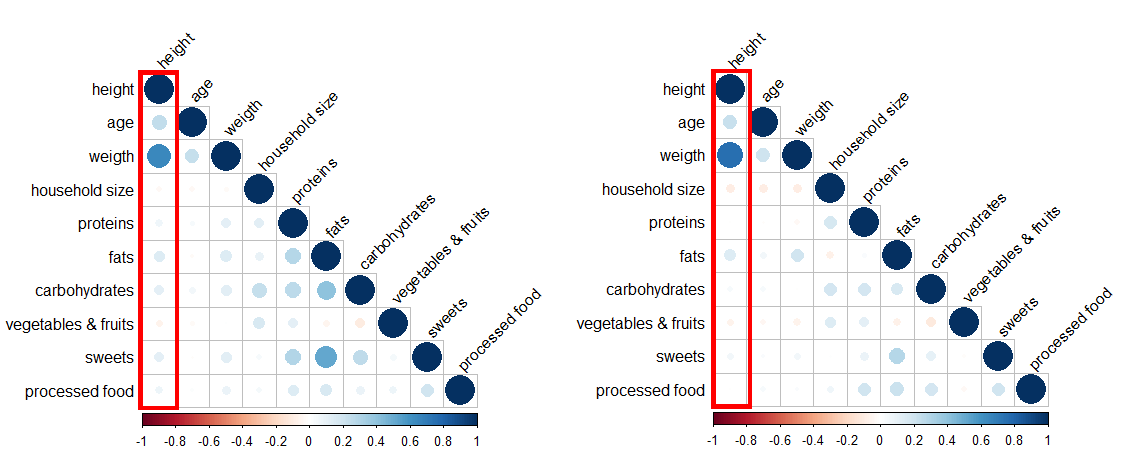
Figure 1 Association of height and different nutritional components of 5-year-old (left)
and 12-year-old (right) Ethiopian children (n = 2000) measured longitudinal between
2006–2012. Strength of colors indicates the strength of the association (blue: positive,
red: negative).
We also re-analyzed anthropometric measurements of the Kolkata Growth Study, India. This
study took place in 1982–1983, with data on 825 Bengali boys aged 7 to 16 years (KG1). A
second Kolkata Growth Study (KG2) was performed between 1999 and 2011, with data of 1999
boys aged 7 to 21 years from Bengali Hindu families, and between 2005 and 2011, with data of
2195 girls (Scheffler et al. 2018).
The number of stunted children slightly decreased between KG1 and KG2. Mean values standard
deviation scores of body height (hSDS) of boys increased from -0.71 hSDS in 1982 to -0.49
hSDS in 2011, and as the BMI also increased from -1.4 SDS to -0.29 SDS, these data were
originally interpreted as evidence of improved nutritional conditions. Yet, this impression,
though in line with accepted knowledge, is false.
Figure 2 illustrates the association between body
height and skinfold thickness in a subpopulation of boys of the 2011 Kolkata Growth study
(KG2). Evidently, height is not associated with skinfold thickness. The same was true for
measurements obtained in KG1.

Figure 2 Association of skinfold thickness on triceps (SDS, Indian reference) and height
(SDS, reference WHO) of 1,900 Indian boys 2011 (Multiple Regression, CI (99%):
-0.011/0.106, p > 0.001). Measurements below the red line indicate
stunting.
Similar results were obtained in a 2018 study in Indonesia performed on three Islands
(Bali, West-Timor, Sumatra) in rural and urban areas (Scheffler et al. 2020). Indonesian children lack relevant associations between
skinfold thickness (x̅SF-mean of subscapular and triceps skinfold) and body height (hSDS).
Rural boys of Soe (West-Timor) were shortest (hSDS = -2.08), and thinnest (BMI_SDS = -1.41),
closely followed by the girls (hSDS = -1.90; BMI_SDS = -1.25). A total 53% of the boys in
Soe and 46% of the girls in Soe were stunted. Mean skinfold thickness (x̅SF: boys 5.50 mm,
girls 6.72 mm) was significantly less than in the urban children of Kupang, the capital of
West-Timor (x̅SF: boys 7.65 mm, girls 8.75 mm). Even though the very thin children of Kupang
were slightly shorter, they were still significantly taller than the children of Soe. The
correlation between x̅SF and hSDS ranged from r = 0.12 to r = 0.38, explaining a maximum of
14.4% of the hSDS variance.
Even though the prevalence of stunting was up to 53% in the Indonesian population and thus
much higher than in the Kolkata study, the association between body height and
nutrition-related anthropometric measurements was negligible. This was also the case for BMI
and MUAC.
A second study in Kupang in 2020 highlighted the impact of the social strata on body height
and skinfold thickness (Scheffler et al. 2021a).
Figure 3 shows that affluent children from a
Catholic private school were significantly taller than disadvantaged children from the
underprivileged school, and they had higher subcutaneous fat layers. The prevalence of
stunting in boys was 8.5%, 26.4%, and 46.8% (private school, state schools, and
underprivileged school). The prevalence of stunting in girls was 10.4%, 20.3%, and 25.5%,
respectively. At first glance, these data appear to confirm the current perception that
higher BMI, higher skinfold thickness, and larger MUAC yield better growth. Yet, figure 3 highlights that the association between body
height and skinfold thickness becomes negligible when studied within each group of children
separately. Stunted children are found in all social strata, regardless of skinfold
thickness.
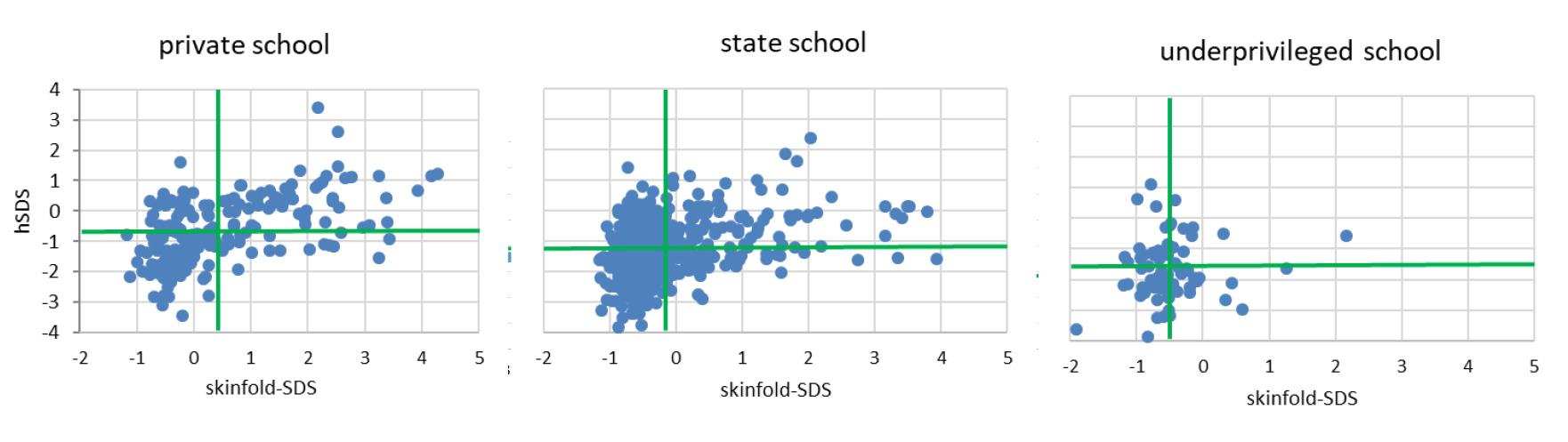
Figure 3 Height (hSDS, reference WHO) and mean skinfold thickness [(subscapular +
triceps)/2; skinfold-SDS, reference these data set] of 723 children from urban
Kupang/West-Timor, Indonesia. 196 children from a Catholic private school, 452 children
from public state schools, and 75 children from an underprivileged school of the
suburban region. Green horizontal lines indicate mean hSDS, green vertical lines
indicate mean skinfold-SDS of each school.
The lack of association between body length, weight, and body mass index is well known.
Figure 4 was obtained from (Prentice et al. 2013) and shows early infant patterns of weight for
age, weight for length, and length for age in 54 studies from LMIC. Whereas infants
significantly drop in length-for-age up to age 2 years, they remain appropriate in
weight-for-length.

Figure 4 Mean anthropometric z-scores (hSDS-HAZ, wSDS-WAZ, height-for-length SDS-WHZ) for
54 studies from low- and middle-income countries relative to the WHO standard (Prentice et al. 2013) (reprinted with kind
permission of Oxford University Press, November 30th 2020)
Recently published data from India (Subramanian et al.
2020) support that anthropometric failure is not strongly associated with measures
of 31 nutritional indicators. The stunting rate of different regions in India does not
coincide with the inadequate diet (Fig. 5). Districts
with high prevalence of stunting, e.g., West Bengal and the Western provinces of India, do
not always show highest prevalence of inadequate diet.

Figure 5 Prevalence of stunted children and inadequate diet in the different districts of
India. Prevalence-headcount-metric included prevalence and absolute headcount number.
(Subramanian et al. 2020) (General
permission: CC0 1.0 Universal (CC0 1.0) Public Domain Dedication)
In summary, there is strong evidence that stunting and malnutrition are different entities.
Stunting is often associated with but not specific for poverty, poor health, and
malnutrition. Malnutrition can lead to stunting, but the reverse equation is not true:
Stunting is not a synonym of malnutrition.
But why are the children in the LMIC (Black et al.
2013) so frequently stunted?
Stunting is a synonym of social disadvantage and poor parental education
Humans are social, they have a species-specific basic pattern of growth (Bogin et al. 2018b; Bogin 1999; Bogin 2020) as an outcome of
the four- to seven-million-year evolutionary history of the hominins. The bio-cultural
nature of our species includes a prolonged childhood and allows for intense learning and
adapting social behavior from adults. Children and adolescents are capable of recognizing
their own social position among their peers and within society. Social, political, and
emotional interactions are not limited to structuring living conditions and the psychosocial
environment but also have an important influence on physical growth, development, and
cognitive maturation. Panter-Brick (1998), Bogin
(Bogin 1999; Bogin 2020; Bogin 2021), and numerous
other authors addressed that psychosocial well-being and stress are dimensions of an
individual’s health with physiological responses in behavior and also in endocrine
regulation. Stress hormone levels are negatively associated with social strata (Ursache et al. 2015; Zilioli et al. 2017).
Body height (next to age at menarche) has traditionally been considered a measure of the
quality of living conditions (Tanner 1987). It has
become common practice in economic history, demography, public health, and political policy
inquiry to take body height as an appropriate measure of living conditions. Shorter height
is associated with less education (Fig. 6, lower
social status, and income (Bogin 1999; Bogin et al. 2002; Hermanussen and Scheffler 2016; NCD Risk Factor
Collaboration 2016). These associations suggest positive feedback between greater
height and better living conditions. Nevertheless, what is the implication of better living
conditions on body height?
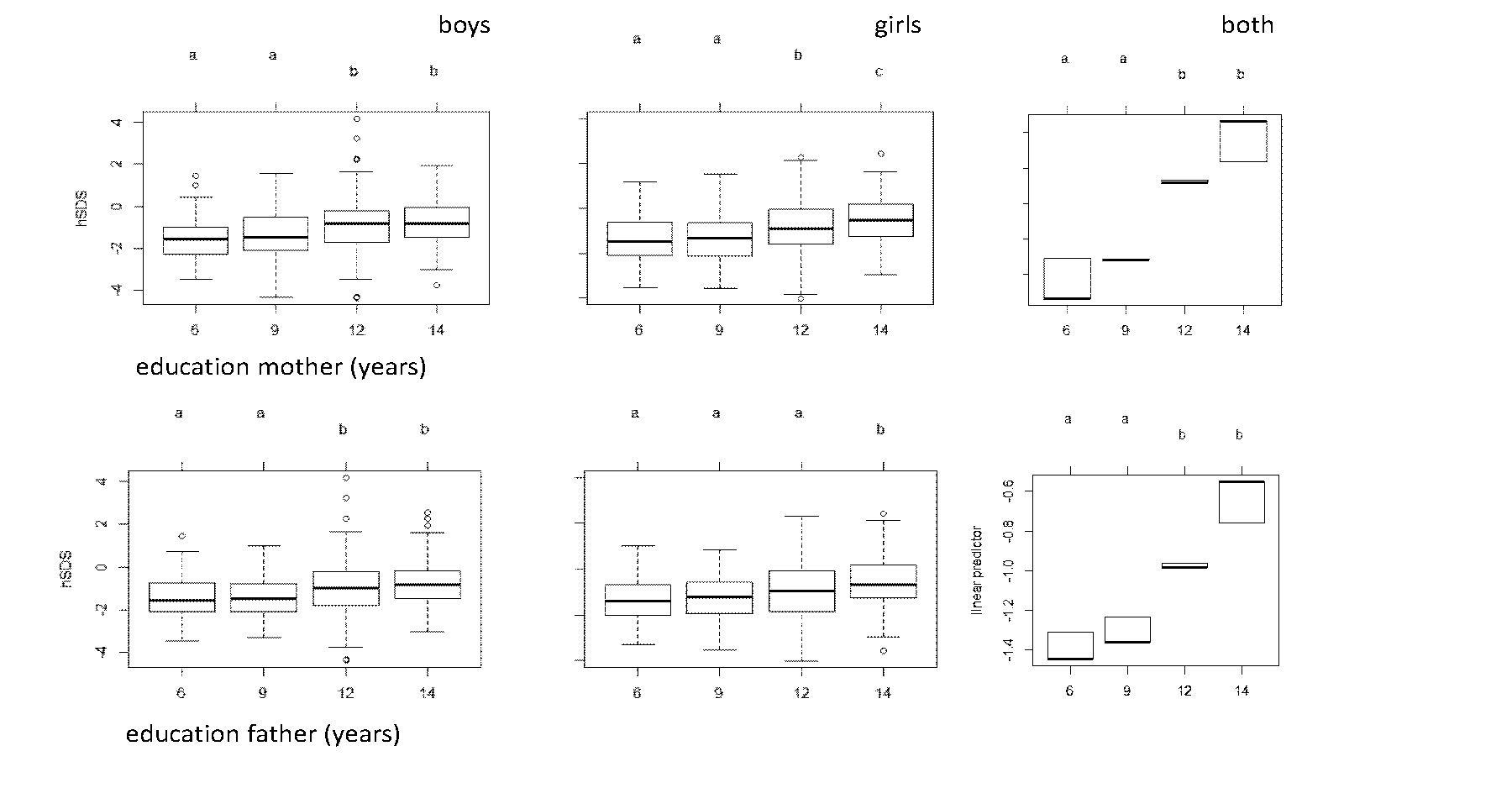
Figure 6 Body height (hSDS) of 6–13-year-old children of Indonesia depending on mothers’
and fathers’ education (years of education) and the linear prediction (ANOVA; mother F =
32.69, p < 0.000, father F = 24.06, p < 0.000; a, b, c indicate significant
differences between adjoining groups)
In many social species, size is associated with social position within the group and mating
success. This has, for example, been shown for baboons, deer, and meerkats (Bercovitch and Clarke 1995; Cowlishaw and Dunbar 1991; Huchard
et al. 2016; Waal 1986). Stature itself is
a lifelong social signal. Social interactions and group behavior are modulated by body
height and, in turn, are able to modulate body height, allowing competitive growth and
strategic growth adjustments similar to what has been shown in meerkats (Huchard et al. 2016). There is a common perception that
large body size and tall stature result in social dominance (Cinnirella and Winter 2009; Hermanussen and Scheffler 2016). This also applies to humans. Humans are able to
perceive physical size as a signal of social dominance. Huang et al. (2002) have described the greater influence of humans perceived as
taller in a negotiation task. Taller men are perceived as more competent and authoritative
(Cinnirella and Winter 2009; Judge and Cable 2004). Also, children are able to
recognize cues that predict dominance (Lourenco et al.
2015). They recognize the physical size of individual members of a group and
numerical alliances as signals of social hierarchies. Groups of children from socially
dominant backgrounds are educated both formally and by social experience to anticipate
future dominance (Clark and Cummins 2014) while
others anticipate subordination (Hermanussen and Scheffler
2016).
Education is important. The educational level of parents has a positive influence on body
height. The above-discussed anthropometric studies of stunted children in India and
Indonesia also provided information on social background and on parental education. Figure 6
shows that parental education (number of years spent in school and university) was
positively associated with body height of the children from a study, which was conducted in
different regions in Indonesia (Bali, West-Timor and Sumatra) in 2018 and included more than
1,700 primary school children aged between 6 and 13 years (Scheffler et al. 2020).
Body height differs according to school type (Figure 3). On average, wealthy parents of
private school children spent 12.35 years in school, whereas parents of state and
underprivileged school children only spent 11.15 and 8.7 years respectively. The influence
of parental education on growth and educational performance (school grades) was strongest in
the girls of the underprivileged school, weaker in state schoolchildren of both sexes, and
weakest in the private school boys. This strongly underlines the significance of parental
education, particularly in the girls of the poorest socio-economic strata. The findings are
in line with evidence that maternal and paternal education were independently associated
with 0.37 (95% CI 0.33 to 0.41) and 0.20 (95% CI 0.16 to 0.24) higher hSDS, and 0.31 (95% CI
0.29 to 0.34) and 0.16 (95% CI 0.14 to 0.18) higher Early Childhood Development Index
z-scores, respectively (comparing secondary or higher to no education), as summarized by
Jeong et al. (2018). The factor household
prosperity, even though associated with parental education (Vaivada et al. 2020), appeared to have no direct impact on height in
either school type. In 2020, in the study of Kupang, additional information on water supply
as well as television and refrigerator access was condensed to a “household score”. The
household score of children attending the private school is significantly better than of
those attending the underprivileged school (p < 0.000). Additionally, poor children are
physically fitter. They showed the best results in standing jump.Their high skeletal
robusticity (high Frame index: elbow breath/height) (Scheffler and Hermanussen 2021) suggested persistent high levels of daily ph
ysical activity (Rietsch et al. 2013).
The shortness of the children of the underprivileged school was neither associated with
clinical signs of malnutrition nor with thinness nor with delay in physical development,
indicating that the shortness in height of underprivileged children is not associated with
poor nutrition (Scheffler et al. 2021a). We only
found significant though small associations between body height and indicators of the state
of nutrition, such as BMI, MUAC, and skinfold thickness, in the wealthy children. It seems
that it is not the poor nutrition that inhibits growth but the abundant nutrition that leads
to accelerated developmental tempo (Hermanussen and
Scheffler 2022) and, in consequence, to taller-than-average body height.
Bogin (Bogin 2020; Bogin 2021) summarized non-nutritional impact on growth in the
Social-Economic-Political-Emotional (SEPE) factors. SEPE factors refer toprestige,
dominance-subordination, social identity, and ego motivation of individuals and groups in a
society. The underprivileged children are socially, economically, politically, and
emotionally disadvantaged (Adriany and Tesar 2022).
This is in line with their lower educational possibilities. A test of self-confidence was
also a part of the above-mentioned study in Indonesia in 2020. We set out to test the
self-confidence as well as the subjective feeling of inferiority of father’s social position
as an emotional influence on growth with the MacArthur Scale of Subjective Social Status
(SSS) but failed, as our Western cultural concepts appear inappropriate when testing
schoolchildren in West Timor, Indonesia (Boeker et al.
2021).
The perception of one’s own social, economic, and emotional position depends on one’s
cultural and time-specific role within society. The influence of self-perception and of
social status becomes particularly evident when people leave one and integrate into another
social network. Migrants are challenged by their new host society and its specific social
roles. Besides the cultural (acquisition of knowledge and skills), the structural (degree of
education, employment), and the social dimension (social relationships) emotional aspects
become increasingly important for their integration (Esser
2006). The emotional dimension includes emotional integration and identification in
line with a personal sense of belonging to society. This is a challenge for migrant children
and they react with phenotypic plasticity in growth and maturation. Migrant children and
adolescents of lower social status rapidly adjust in height towards the average height of
their hosts (Scheffler et al. 2021b). They also
tend to mature earlier and are prone to overweight (Bogin
et al. 2018a). Observations on intergenerational upward and downward social
mobility reflect the strong association between social position and body height: Upward
social mobility results in taller stature, whereas children from “upper class” families who
lose their social advantage tend to end up shorter (Koziel
et al. 2019). Recent evidence links social competition and its effect on
hierarchies in social structures with the neuronal networks of the ventromedial hypothalamus
and body size; the link between size and status permits adaptive plasticity, competitive
growth, and strategic growth adjustments also in humans (Hermanussen et al. 2022).
Conclusion
Stunting is not a synonym of under- or malnutrition. Stunting in the modern sense has been
the natural condition of human height for more than 10.000 years. Already historic
observations on children of starving populations in Europe emphasized the lack of
association between starvation and long-term growth. Modern studies in low-and-middle-income
countries similarly fail to provide evidence of an association between stunting and
malnutrition. Being shorter than average reflects poor social, economic, political, and
emotional circumstances and reflects social disadvantage and poor parental education.
Parental education has a positive effect on the body height of children. The concept of SEPE
is a modern concept explaining the regulation of body height.
References
Adriany, V./Tesar, M. (2022). Unpacking the
discourses of stunting in Indonesian early childhood education and parenting. Children
& Society 37 (2), 311–325. https://doi.org/10.1111/chso.12593.
Antonov, A. N. (1947). Children born during The
Siege of Leningrad in 1942. The Journal of Pediatrics 30 (3), 250–259. https://doi.org/10.1016/s0022-3476(47)80160-x.
Behrman, R. E./Kliegman, R. M./Jenson, H. B.
(1999). Nelson textbook of pediatrics. 16th ed. Philadelphia, London, Toronto,
Saunders.
Beluska-Turkan, K./Korczak, R./Hartell, B./Moskal,
K./Maukonen, J./Alexander, D. E./Salem, N./Harkness, L./Ayad, W./Szaro, J./Zhang,
K./Siriwardhana, N. (2019). Nutritional gaps and supplementation in the first 1000 days.
Nutrients 11 (12), 2891. https://doi.org/10.3390/nu11122891.
Bercovitch, F. B./Clarke, A. S. (1995). Dominance
rank, cortisol concentrations, and reproductive maturation in male rhesus macaques.
Physiology & Behavior 58 (2), 215–221. https://doi.org/10.1016/0031-9384(95)00055-n.
Black, R. E./Victora, C. G./Walker, S. P./Bhutta,
Z. A./Christian, P./Onis, M. de/Ezzati, M./Grantham-McGregor, S./Katz, J./Martorell,
R./Uauy, R./Maternal and Child Nutrition Study Group (2013). Maternal and child
undernutrition and overweight in low-income and middle-income countries. The Lancet 382
(9890), 427–451. https://doi.org/10.1016/S0140-6736(13)60937-X.
Boeker, S./Hermanussen, M./Scheffler, C. (2021).
Westernization of self-perception in modern affluent Indonesian school children. Human
Biology and Public Health 1. https://doi.org/10.52905/hbph.v1.4.
Bogin, B. (1999). Patterns of human growth. 2nd
ed. Cambridge, Cambridge University Press.
Bogin, B. (2020). Patterns of human growth. 3rd
ed. Cambridge, Cambridge University Press.
Bogin, B. (2021).
Social-Economic-Political-Emotional (SEPE) factors regulate human growth. Human Biology
and Public Health 1. https://doi.org/10.52905/hbph.v1.10.
Bogin, B./Hermanussen, M./Scheffler, C. (2018a).
As tall as my peers – similarity in body height between migrants and hosts.
Anthropologischer Anzeiger 74 (5), 363–376. https://doi.org/10.1127/anthranz/2018/0828.
Bogin, B./Smith, P./Orden, A. B./Varela Silva, M.
I./Loucky, J. (2002). Rapid change in height and body proportions of Maya American
children. American Journal of Human Biology 14 (6), 753–761. https://doi.org/10.1002/ajhb.10092.
Bogin, B./Varea, C./Hermanussen, M./Scheffler, C.
(2018b). Human life course biology: A centennial perspective of scholarship on the human
pattern of physical growth and its place in human biocultural evolution. American
Journal of Physical Anthropology 165 (4), 834–854. https://doi.org/10.1002/ajpa.23357.
Boyden, J. (2022). Young lives: an international
study of childhood poverty: round 2, 2006. 4th ed. UK Data Service, SN: 6852. https://doi.org/10.5255/UKDA-SN-6852-4.
Cinnirella, F./Winter, J. (2009). Size matters!
Body height and labor market discrimination: A Cross-European analysis. CESifo Working
Papers 2733, 1–29. Available online at http://hdl.handle.net/10419/30617 (accessed 2/13/2023).
Clark, G./Cummins, N. (2014). Surnames and social
mobility in England, 1170–2012. Human Nature 25 (4), 517–537. https://doi.org/10.1007/s12110-014-9219-y.
Cowlishaw, G./Dunbar, R. I. M. (1991). Dominance
rank and mating success in male primates. Animal Behaviour 41 (6), 1045–1056. https://doi.org/10.1016/S0003-3472(05)80642-6.
Dikanski, M. (1914). Über den Einfluss der
sozialen Lage auf die Körpermaße von Schulkindern. München, Müller &
Steinicke.
Esser, H. (2006). Sprache und Integration:
Konzeptionelle Grundlagen und empirische Zusammenhänge. KMI Working Papers 7. Vienna,
Austrian Academy of Sciences, Commission for Migration and Integration
Research.
Fredriks, A. M./van Buuren, S./Burgmeijer, R.
J./Meulmeester, J. F./Beuker, R. J./Brugman, E./Roede, M. J./Verloove-Vanhorick, S.
P./Wit, J. M. (2000). Continuing positive secular growth change in the Netherlands
1955–1997. Pediatric Research 47 (3), 316–323. https://doi.org/10.1203/00006450-200003000-00006.
Gassner, U. K. (1862). Über die Veränderungen des
Körpergewichts bei Schwangeren, Gebärenden und Wöchnerinnen. Monatsschrift für
Geburtskunde und Frauenkrankheiten 19, 1–68.
Gomez, F./Galvan, R. R./Cravioto, J./Frenk, S.
(1955). Malnutrition in infancy and childhood, with special reference to Kwashiorkor.
Advances in Pediatrics 7 (1), 131–169. https://doi.org/10.1016/S0065-3101(22)00438-8.
Goudet, S./Griffiths, P./Bogin, B./Madise, N.
(2017). Interventions to tackle malnutrition and its risk factors in children living in
slums: a scoping review. Annals of Human Biology 44 (1), 1–10. https://doi.org/10.1080/03014460.2016.1205660.
Griffen, A. S. (2016). Height and calories in
early childhood. Economics & Human Biology 20, 55–69. https://doi.org/10.1016/j.ehb.2015.10.004.
Hermanussen, M./Bogin, B./Scheffler, C. (2018).
Stunting, starvation and refeeding: a review of forgotten 19th and early 20th century
literature. Acta Paediatrica 107 (7), 1166–1176. https://doi.org/10.1111/apa.14311.
Hermanussen, M./Erofeev, S./Scheffler, C. (2022).
The socio-endocrine regulation of human growth. Acta Paediatrica 111 (11), 2077–2081.
https://doi.org/10.1111/apa.16504.
Hermanussen, M./Scheffler, C. (2016). Stature
signals status: The association of stature, status and perceived dominance – a thought
experiment. Anthropologischer Anzeiger 73 (4), 265–274. https://doi.org/10.1127/anthranz/2016/0698.
Hermanussen, M./Scheffler, C. (2022). Nutrition,
size, and tempo. Human Biology and Public Health 3. https://doi.org/10.52905/hbph2022.3.37.
Hermanussen, M./Wit, J. M. (2017). How much
nutrition for how much growth? Hormone Research in Paediatrics 88 (1), 38–45. https://doi.org/10.1159/000454832.
Huang, W./Olson, J. S./Olson, G. M. (2002). Camera
angle affects dominance in video-mediated communication. In: CHI '02 Extended abstracts
on human factors in computing systems (CHI EA '02). New York, Association for Computing
Machinery, 716–717. https://doi.org/10.1145/506443.506562.
Huchard, E./English, S./Bell, M. B. V./Thavarajah,
N./Clutton-Brock, T. (2016). Competitive growth in a cooperative mammal. Nature 533
(7604), 532–534. https://doi.org/10.1038/nature17986.
Jeong, J./Kim, R./Subramanian, S. V. (2018). How
consistent are associations between maternal and paternal education and child growth and
development outcomes across 39 low-income and middle-income countries? Journal of
Epidemiology and Community Health 72 (5), 434–441. https://doi.org/10.1136/jech-2017-210102.
Jones, N. (2018). Young lives: an international
study of childhood poverty: round 1, 2002. 6th ed. UK Data Service, SN: 5707. https://doi.org/10.5255/UKDA-SN-5307-3.
Judge, T. A./Cable, D. M. (2004). The effect of
physical height on workplace success and income: preliminary test of a theoretical
model. Journal of Applied Psychology 89 (3), 428–441. https://doi.org/10.1037/0021-9010.89.3.428.
Keys, A./Brožek, J./Henschel, A./Mickelsen,
O./Longstreet Taylor, H. (1950). The biology of human starvation: vol. II. Minneapolis,
University of Minnesota Press.
Koch, E. W. (1935). Über die Veränderung
menschlichen Wachstums im ersten Drittel des 20. Jahrhunderts. Leipzig, Johann Ambrosius
Barth Verlag.
Koziel, S./Zaręba, M./Bielicki, T./Scheffler,
C./Hermanussen, M. (2019). Social mobility of the father influences child growth: A
three-generation study. American Journal of Human Biology 31 (4), e23270. https://doi.org/10.1002/ajhb.23270.
Kristjansson, E./Francis, D. K./Liberato,
S./Benkhalti Jandu, M./Welch, V./Batal, M./Greenhalgh, T./Rader, T./Noonan, E./Shea,
B./Janzen, L./Wells, G. A./Petticrew, M. (2015). Food supplementation for improving the
physical and psychosocial health of socio-economically disadvantaged children aged three
months to five years (Review). Cochrane Database of Systematic Reviews (3), CD009924.
https://doi.org/10.1002/14651858.CD009924.pub2.
Lartey, A. (2015). What would it take to prevent
stunted growth in children in sub-Saharan Africa? The Proceedings of the Nutrition
Society 74 (4), 449–453. https://doi.org/10.1017/S0029665115001688.
Lourenco, S. F./Bonny, J. W./Schwartz, B. L.
(2015). Children and adults use physical size and numerical alliances in third-party
judgments of dominance. Frontiers in Psychology 6, 2050. https://doi.org/10.3389/fpsyg.2015.02050.
Mumm, R./Scheffler, C. (2019). Lack of evidence of
nutritional influence on height in four low and middle-income countries.
Anthropologischer Anzeiger 76 (5), 421–432. https://doi.org/10.1127/anthranz/2019/0988.
NCD Risk Factor Collaboration (2016). A century of
trends in adult human height. eLife 5, e13410. https://doi.org/10.7554/eLife.13410.
Panter-Brick, C. (Ed.) (1998). Biosocial
perspectives on children. Biosocial Society Symposium Series 10. Cambridge, Cambridge
University Press.
Pfaundler, M. (1916). Körpermaß-Studien an
Kindern. Zeitschrift für Kinderheilkunde 14 (1-2), 1–148. https://doi.org/10.1007/BF02225628.
Portrait, F. R. M./van Wingerden, T. F./Deeg, D.
J. H. (2017). Early life undernutrition and adult height: The Dutch famine of 1944–45.
Economics & Human Biology 27 (B), 339–348. https://doi.org/10.1016/j.ehb.2017.09.008.
Prendergast, A. J./Humphrey, J. H. (2014). The
stunting syndrome in developing countries. Paediatrics and International Child Health 34
(4), 250–265. https://doi.org/10.1179/2046905514Y.0000000158.
Prentice, A. M./Ward, K. A./Goldberg, G.
R./Jarjou, L. M./Moore, S. E./Fulford, A. J./Prentice, A. (2013). Critical windows for
nutritional interventions against stunting. The American Journal of Clinical Nutrition
97 (5), 911–918. https://doi.org/10.3945/ajcn.112.052332.
Rietsch, K./Eccard, J. A./Scheffler, C. (2013).
Decreased external skeletal robustness due to reduced physical activity? American
Journal of Human Biology 25 (3), 404–410. https://doi.org/10.1002/ajhb.22389.
Rooij, S. R. de/Wouters, H./Yonker, J. E./Painter,
R. C./Roseboom, T. J. (2010). Prenatal undernutrition and cognitive function in late
adulthood. Proceedings of the National Academy of Sciences (PNAS) 107 (39), 16881–16886.
https://doi.org/10.1073/pnas.1009459107.
Rosenstock, E./Ebert, J./Martin, R./Hicketier,
A./Walter, P./Groß, M. (2019). Human stature in the Near East and Europe ca. 10,000–1000
BC: its spatiotemporal development in a Bayesian errors-in-variables model.
Archaeological and Anthropological Sciences 11 (10), 5657–5690. https://doi.org/10.1007/s12520-019-00850-3.
Scheffler, C./Hermanussen, M. (2021). Stunting
does not impair physical fitness in Indonesian school children. Human Biology and Public
Health 2. https://doi.org/10.52905/hbph.v2.19.
Scheffler, C./Hermanussen, M. (2022). Stunting is
the natural condition of human height. American Journal of Human Biology 34 (5), e23693.
https://doi.org/10.1002/ajhb.23693.
Scheffler, C./Hermanussen, M./Bogin, B./Liana, D.
S./Taolin, F./Cempaka, P. M. V. P./Irawan, M./Ibbibah, L. F./Mappapa, N. K./Payong, M.
K. E./Homalessy, A. V./Takalapeta, A./Apriyanti, S./Manoeroe, M. G./Dupe, F. R./Ratri,
R. R. K./Touw, S. Y./K, P. V./Murtani, B. J./Nunuhitu, R./Puspitasari, R./Riandra, I.
K./Liwan, A. S./Amandari, P./Permatasari, A. A. I./Julia, M./Batubara, J./Pulungan, A.
(2020). Stunting is not a synonym of malnutrition. European Journal of Clinical
Nutrition 74 (3), 377–386. https://doi.org/10.1038/s41430-019-0439-4.
Scheffler, C./Hermanussen, M./Soegianto, S. D.
P./Homalessy, A. V./Touw, S. Y./Angi, S. I./Ariyani, Q. S./Suryanto, T./Matulessy, G. K.
I./Fransiskus, T./Safira, A. V. C./Puteri, M. N./Rahmani, R./Ndaparoka, D. N./Payong, M.
K. E./Indrajati, Y. D./Purba, R. K. H./Manubulu, R. M./Julia, M./Pulungan, A. B.
(2021a). Stunting as a synonym of social disadvantage and poor parental education.
International Journal of Environmental Research and Public Health 18 (3), 1350.
https://doi.org/10.3390/ijerph18031350.
Scheffler, C./Krützfeldt, L.-M./Dasgupta,
P./Hermanussen, M. (2018). No association between fat tissue and height in 5019 children
and adolescents, measured between 1982 and in 2011 in Kolkata/India. Anthropologischer
Anzeiger 74 (5), 403–411. https://doi.org/10.1127/anthranz/2018/0827.
Scheffler, C./Nguyen, T. H./Hermanussen, M.
(2021b). Vietnamese migrants are as tall as they want to be. Human Biology and Public
Health 2. https://doi.org/10.52905/hbph.v2.12.
Schlesinger, E. (1919). Wachstum, Gewicht und
Konstitution der Kinder und der herangewachsenen Jugend während des Krieges. Zeitschrift
für Kinderheilkunde 22 (1), 79–123. https://doi.org/10.1007/BF02087277.
Sguassero, Y./Onis, M. de/Bonotti, A. M./Carroli,
G. (2012). Community-based supplementary feeding for promoting the growth of children
under five years of age in low and middle income countries (Review). Cochrane Database
of Systematic Reviews (6), CD005039. https://doi.org/10.1002/14651858.CD005039.pub3.
Subramanian, S. V./Sarwal, R./Joe, W./Kim, R.
(2020). Geo-visualising diet, anthroprometric and clinical indicators for children in
India (Version 6.0). Harvard Dataverse, UNF:6:UMlPSb5C5m4rnNYf+gPgdw== [fileUNF].
https://doi.org/10.7910/DVN/ZSH8HR.
Tanner, J. M. (1987). Growth as a mirror of the
condition of society: Secular trends and class distinctions. Pediatrics International 29
(1), 96–103. https://doi.org/10.1111/j.1442-200X.1987.tb00015.x.
Uauy, R./Kain, J./Corvalan, C. (2011). How can the
Developmental Origins of Health and Disease (DOHaD) hypothesis contribute to improving
health in developing countries? The American Journal of Clinical Nutrition 94 (Suppl 6),
1759S‐1764S. https://doi.org/10.3945/ajcn.110.000562.
UIA (2022). Inanition. In: The Encyclopedia of
World Problems and Human Potential. Union of International Associations. Available
online at http://encyclopedia.uia.org/en/problem/141425 (accessed
10/19/2022).
Ursache, A./Noble, K. G./Blair, C. (2015).
Socioeconomic status, subjective social status, and perceived stress: Associations with
stress physiology and executive functioning. Behavioral Medicine 41 (3), 145–154.
https://doi.org/10.1080/08964289.2015.1024604.
Vaivada, T./Akseer, N./Akseer, S./Somaskandan,
A./Stefopulos, M./Bhutta, Z. A. (2020). Stunting in childhood: an overview of global
burden, trends, determinants, and drivers of decline. The American Journal of Clinical
Nutrition 112 (Suppl 2), S777–S791. https://doi.org/10.1093/ajcn/nqaa159.
Waal, F. B. M. de (1986). The integration of
dominance and social bonding in primates. The Quarterly Review of Biology 61 (4),
459–479. https://doi.org/10.1086/415144.
Waterlow, J. C. (1972). Classification and
definition of protein-calorie malnutrition. British Medical Journal 3 (5826), 566–569.
https://doi.org/10.1136/bmj.3.5826.566.
Waterlow, J. C. (Ed.) (1988). Linear growth
retardation in less developed countries. Nestlé Nutrition Workshop Series 14. New York,
Raven Press.
WHO (2021). Fact sheet: Malnutrition. Available
online at https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed
9/30/2022).
WHO (2022). Mother and newborn information for
tracking outcomes and results (MoNITOR). Available online at https://www.who.int/groups/mother-and-newborn-information-for-tracking-outcomes-and-results-(monitor)
(accessed 2/3/2023).
Wilke, L./Böker, S./Mumm, R./Groth, D. (2021).
Social status influences human growth. A summary and analysis of historical data from
German school girls in 1914 with comparison to modern references. Human Biology and
Public Health 3. https://doi.org/10.52905/hbph2021.3.22.
Woldehanna, T./Sanchez, A./Penny, M./Duc, L.
T./Boyden, J. (2018). Young lives: an international study of childhood poverty: round 4,
2013–2014. 2nd ed. UK Data Service, SN: 7931. https://doi.org/10.5255/UKDA-SN-7931-2.
Zilioli, S./Slatcher, R. B./Fritz, H./Booza, J.
C./Cutchin, M. P. (2017). Brief report: Neighborhood disadvantage and hair cortisol
among older urban African Americans. Psychoneuroendocrinology 80, 36–38. https://doi.org/10.1016/j.psyneuen.2017.02.026.