The dilemma of misclassifying weight in short and in historic
population
Rebekka Mumm ✉
✉
University of Potsdam, Human Biology, 14469 Potsdam, Germany
Michael Hermanussen
Aschauhof, 24340 Eckernförde-Altenhof, Germany
DOI: https://doi.org/10.52905/hbph2021.3.28
Abstract
Background
Clinicians often refer anthropometric measures of a child to so-called “growth
standards” and “growth references. Over 140 countries have meanwhile adopted WHO growth
standards.
Objectives
The present study was conducted to thoroughly examine the idea of growth standards as a
common yardstick for all populations. Weight depends on height. We became interested in
whether also weight-for-height depends on height. First, we studied the age-group effect
on weight-for-height. Thereafter, we tested the applicability of weight-for-height
references in short and in historic populations.
Sample and Methods
We analyzed body height and body weight and weight-for-height of 3795 healthy boys and
3726 healthy girls aged 2 to 5 years measured in East-Germany between 1986 and 1990.
We chose contemporary height and weight charts from Germany, the UK, and the WHO growth
chart and compared these with three geographically commensurable growth charts from the
end of the 19th century.
Results
We analyzed body height and body weight and weight-for-height of 3795 healthy boys and
3726 healthy girls aged 2 to 5 years measured in East-Germany between 1986 and 1990.
We chose contemporary height and weight charts from Germany, the UK, and the WHO growth
chart and compared these with three geographically commensurable growth charts of the
end of the 19th century.
Conclusion
Weight-for-height depends on age and sex and apart from the nutritional state, reflects
body proportion and body built particularly during infancy and early childhood.
Populations with a relatively short average height are prone to high values of
weight-for-height for arithmetic reasons independent of the nutritional state.
Keywords: growth standards, growth references, body mass index, nutritional status
Conflict of Interest: There are no
conflicts of interest.
Citation: Mumm, R. / Hermanussen, M. (2021). The dilemma of misclassifying weight in short and in historic
population. Human Biology and Public Health 3. https://doi.org/10.52905/hbph2021.3.28.
Copyright: This is an open access article distributed under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11-01-2022 | Accepted: 31-03-2022 | Published: 16-06-2022
Take home message for students
Weight-for-height reflects the variation in body proportion and body built, particularly
early in life. At a young age, short children have lower weight-for-height z-scores than
tall children of the same age. Weight-for-height does not solely characterize the
nutritional state. Particularly short populations are prone to high weight-for-height for
arithmetic reasons.
Contents
Introduction
Clinicians often refer anthropometric measures of a child to so-called “growth standards”
and “growth references”. Growth standards and references are based on samples of children
that are considered healthy, normally developed, and representative for the variables of
interest. In recent years, World Health Organization (WHO) standards and references for
height and weight, and also for body mass index (BMI) and weight-for-height (WHO 2006) have been widely used in public health and
medicine and by governmental and health organizations for monitoring the well-being of
children. The latter is of particular interest because already in 1973 it was stated that
“the expected weight of a child of given height is independent of age and largely
independent of race” (Waterlow 1973). Over 140
countries have meanwhile adopted WHO growth standards. United Nations agencies use WHO
growth standards and references as the “common yardstick to assess and monitor child growth”
(Zorlu 2011).
The present study was conducted to thoroughly examine the idea of growth standards as a
common yardstick for all populations. It is unquestionable that weight depends on height.
Taller people tend to be the heavier people. However, we became interested in the question
of whether also weight-for-height depends on height. First, we studied the age-group effect
on weight-for-height. Thereafter, we tested the applicability of weight-for-height
references in short and in historic populations.
The age group effect
In groups of children of different ages (“mixed-age” groups), the youngest children are
usually the shortest and lightest ones. The same applies to groups of children of the same
age (“same-age” groups). Also in these groups, the shorter children tend to be the lighter
children. Referring weight to height can be done in two ways: either within groups of
children of different ages (“mixed-age” groups) or in groups of children of the same age
(“same-age” groups). The commonly used modern weight-for-height reference tables published
by the Centers for Disease Control and Prevention CDC (CDC 2001; Kuczmarski et al. 2002) and
WHO (WHO 2006) are “mixed-age” tables for boys
and girls aged 2 to 5 years.
Children differ in proportion. Young children have greater sitting height, and appear
more “robust” than older children (Mumm et al.
2018; Schüler 2009). In “mixed-age”
groups of children of the same height, the younger children tend to be the
heaviest-for-height for reasons of proportion and robusticity. On the other hand, for the
same reason in “same-age” groups, the shorter children should tend to have the least
weight-for-height. We hypothesize that the shortest children of “same-age” groups will
have the lowest weight-for-height z-scores.
Historic weight-for-height
Since the end of the 19th century, height and weight of European children of all ages has
increased significantly. Similar trends in size have meanwhile been observed in many
countries throughout the world. Yet, as height and weight tend to change with each other,
we hypothesize that despite the obvious trend in size, the ratio weight-for-height has
remained unchanged in recent history.
Sample and Method
We analyzed body height and body weight of 3795 healthy boys and 3726 healthy girls aged 2
to 5 years measured in East-Germany between 1986 and 1990. Details of this investigation
were published elsewhere (Greil 1988). We calculated
weight-for-height, and weight-for-height z-scores based on WHO growth standards (WHO 2006).
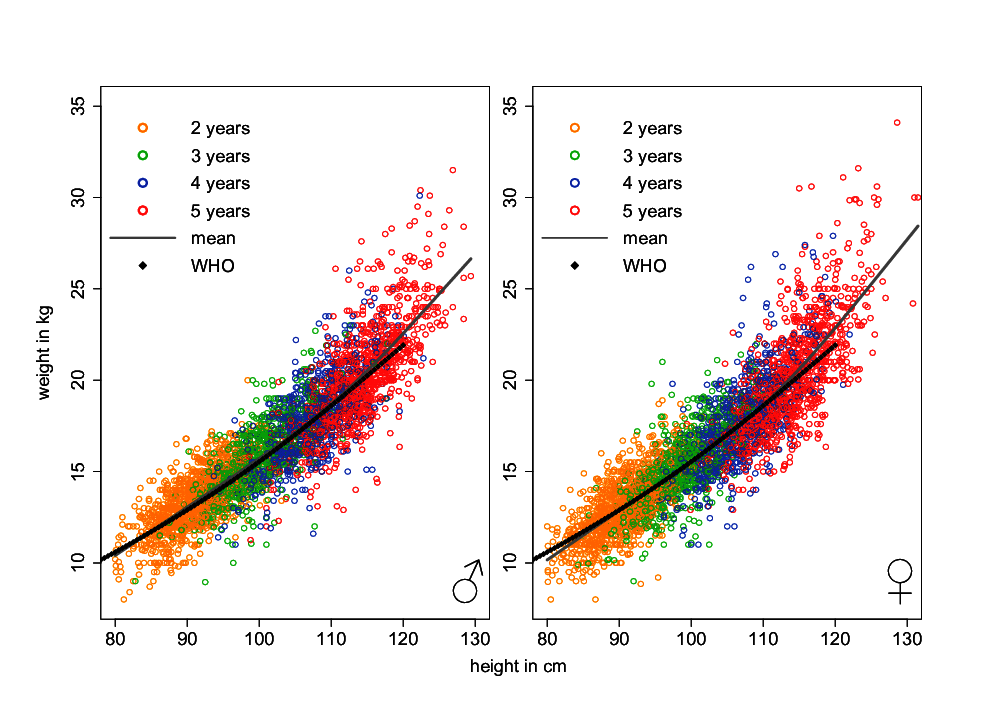
Figure 1 Weight-for-height in healthy East German boys and girls aged 2 to 5 years. Colors
indicate the different age classes. The grey line indicates mean values of
weight-for-height of the German sample. Black diamonds show mean values of
weight-for-age referred to mean values of height-for-age of the WHO growth standards
(WHO
2006).
In addition, we chose contemporary height and weight charts of 2-to-10-year-old boys from
Germany (Neuhauser et al. 2013), the UK (Freeman et al. 1995), and the WHO growth chart (WHO 2006), and compared these with three commensurable
growth charts from the 19th century (Germany (Camerer
1893), England (1890 after (Weissenberg
1911), p.170) and 5-to-10-year-old boys from Boston, USA (Bowditch 1877)). All analyses were done with the statistical software R
(R Core Team 2021).
Results
Weight depends on height. Figure 1 illustrates the relation between height and weight in
healthy East German boys and girls aged 2 to 5 years. In each age group, the shortest
children are the lightest children. Mean values of weight for height are indicated. Black
diamonds show mean values of weight-for-age referred to the corresponding mean
height-for-the same age obtained from the WHO growth standards (WHO 2006). The figure highlights the similarity between the German
curve, and the pattern obtained from the WHO standard.
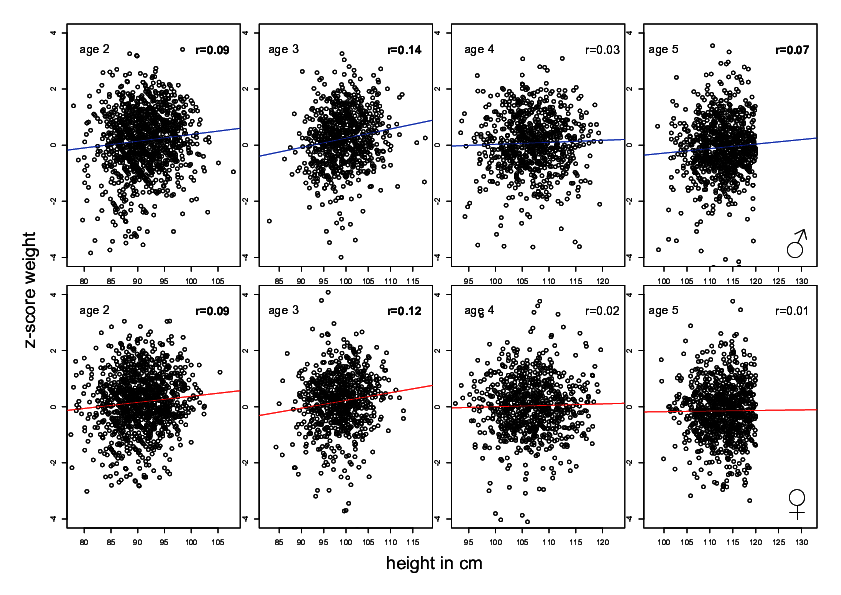
Figure 2 Weight-for-height z-scores (WHO growth standards (WHO 2006) referred to height at age 2 to 5 years. Short-for-age children tend
to have lower weight z-scores than tall-for-age children of the same age. Significant
Pearson-correlations in bold.
Figure 2 refers z-scores of weight-for-height based on WHO growth standards (WHO 2006) to height. The figure illustrates that in
“same-age” groups, the shorter children tend to be lighter-for-height than the taller
children. This feature is significant as it reflects age-related differences in body
proportion and body built. Yet, the effect is small with correlation coefficients (Pearson
correlation) between r=0.02 and r=0.14, and may be ignored for practical reasons. This is
however different in historic settings.
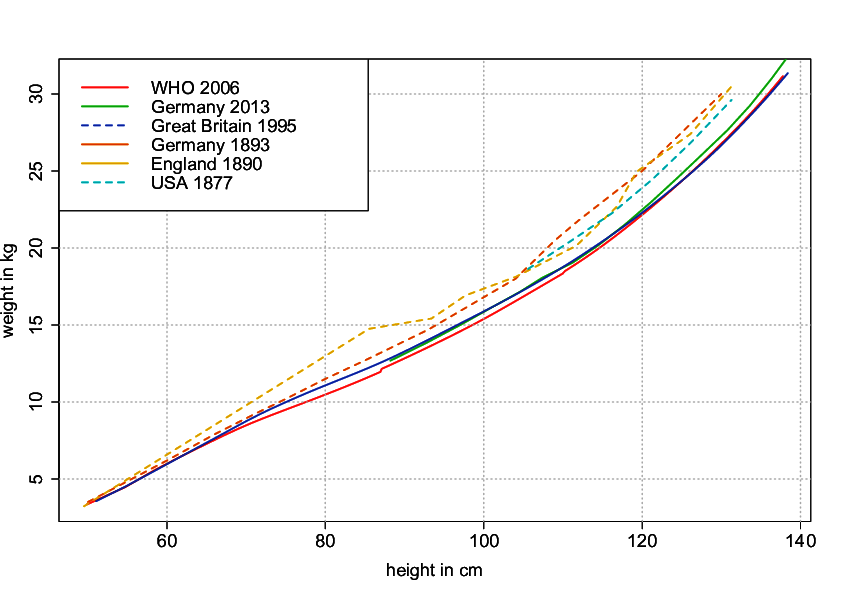
We visualized mean weight-for-height in contemporary and historic data by plotting mean
values of weight-for-age against the corresponding mean values of height-for-the-same-age.
Figure 3 illustrates mean weight-for-height of three contemporary and three historic growth
charts of similar ethnic background. Historic weight-for-height ranges significantly above
contemporary weight-for-height. Beyond body heights of some 80 cm, historic-children were up
to 3 kg heavier than contemporary-children of the same height.
Discussion
Weight-for-age depends on height-for-age with a coefficient of correlation close to r=0.7
(Mumm and Hermanussen 2021).
Weight-for-height depends on age and sex, and apart from the nutritional state, reflects
body proportion and body built particularly during infancy and early childhood. Our first
hypothesis that short children of “same-age” groups have lower weight-for-height z-scores
than tall children of the same age appears true. This is contrary to the statement of
Waterlow that “the expected weight of a child of given height is independent of age and
largely independent of race” (Waterlow 1973).
However, the effect is small and of questionable practical relevance. Thus, for practical
reasons, weight-for-height references may ignore the age factor.
Contemporary references of weight-for-height resemble each other. Even weight-for-height of
East German children measured some 40 years ago is strikingly similar to the contemporary
weight-for-height reference tables published by the Centers for Disease Control and
Prevention (Kuczmarski et al. 2002; CDC 2001) and WHO (WHO
2006). This was different at the end of 19th century. Previous European
populations were shorter (Scheffler and Hermanussen
2021; Hermanussen et al. 2018). As child
obesity was not an issue in those days, the children were certainly not “too heavy for their
body height”, rather “too short for their weight”. Weight-for-height has significantly
changed throughout recent history with up to 3 kg less weight in contemporary children of
the same height. We thus reject the second hypothesis. Weight-for-height is sensitive to
secular changes. Short populations are prone to high values of weight-for-height for
arithmetic reasons independent of the nutritional state. The data highlight the effect of
stature on the weight-for-height ratio and emphasize that by no means weight-for-height
solely characterizes the nutritional state.
Additional studies are in progress which focus on similar arithmetic problems when using
BMI for classifying the nutritional status of populations that differ in height from the
references they are referred to. Preliminary data suggest that currently used critical
cut-off values of BMI for defining “thinness”, “overweight” and “obesity” (Cole and Lobstein 2012) (Nutrition Landscape Information System 2022) may lead to serious
clinical misinterpretations (Hermanussen et al.
2022).
Conclusion
Weight-for-height depends on age and sex, and apart from the nutritional state, reflects
body proportion and body built particularly during infancy and early childhood. Populations
with a relatively short average height are prone to high values of weight-for-height for
arithmetic reasons independent of the nutritional state.
Acknowledgements
The manuscript is the result of our participation in the International Student Summer
School “Statistical Approaches to the Developmental and Growth Data of Children and
Adolescents” in Gülpe from July 18th to 24th, 2021. The Summer School was supported by the
Auxological Society (Deutsche Gesellschaft für Auxologie), the Society of Anthropology
(Gesellschaft für Anthropologie) and KoUP funding of University of Potsdam, Germany.
References
Bowditch, H. P. (1877). Growth of children:
Eightth annual report of the State Board of Health of Massuchusetts.
Boston.
Camerer, W. (1893). Untersuchungen über
Massenwachstum und Längenwachstum der Kinder. Jahrbuch der Kinderheilkunde Neue Folge
36, 249–293.
CDC (2001). Data Table of Weight-for-stature
Charts 2001. Available online at https://www.cdc.gov/growthcharts/html_charts/wtstat.htm#females (accessed
1/7/2022).
Cole, T. J./Lobstein, T. (2012). Extended
international (IOTF) body mass index cut-offs for thinness, overweight and obesity.
Pediatric obesity 7 (4), 284–294. https://doi.org/10.1111/j.2047-6310.2012.00064.x.
Freeman, J. V./Cole, T. J./Chinn, S./Jones, P.
R./White, E. M./Preece, M. A. (1995). Cross sectional stature and weight reference
curves for the UK, 1990. Archives of disease in childhood 73 (1), 17–24. https://doi.org/10.1136/adc.73.1.17.
Greil, H. (1988). Der Körperbau im
Erwachsenenalter. Berlin, Humboldt-University.
Hermanussen, M./Bogin, B./Scheffler, C. (2018).
Stunting, starvation and refeeding: a review of forgotten 19th and early 20th century
literature. Acta paediatrica (Oslo, Norway : 1992) 107 (7), 1166–1176. https://doi.org/10.1111/apa.14311.
Hermanussen, M./Novine, M./Scheffler, C./Groth, D.
(2022). The arithmetic dilemma when defining thinness, overweight and obesity in stunted
populations. Human Biology and Public Health in print.
Kuczmarski, R. J./Ogden, C. L./Guo, S.
S./Grummer-Strawn, L./Flegal, K. M./Mei, Z./Wei, R./Curtin, L. R./Roche, A. F./Johnson,
C. L. (2002). 2000 CDC Growth Charts for the United States: methods and development.
Vital and health statistics. Series 11, Data from the National Health Survey (246),
1–190.
Mumm, R./Godina, E./Koziel, S./Musalek, M./Sedlak,
P./Wittwer-Backofen, U./Hesse, V./Dasgupta, P./Henneberg, M./Scheffler, Ch. (2018).
External skeletal robusticity of children and adolescents - European references from
birth to adulthood and international comparisons. Anthropologischer Anzeiger; Bericht
uber die biologisch-anthropologische Literatur 74 (5), 383–391. https://doi.org/10.1127/anthranz/2018/0826.
Mumm, R./Hermanussen, M. (2021). A short note on
the BMI and on secular changes in BMI. Human Biology and Public Health 2. https://doi.org/10.52905/hbph.v2.17.
Neuhauser, H./Schienkiewitz,
A./Schaffrath-Rosario, A./Dortschy, R./Kurth, B.-M. (2013). Referenzperzentile für
anthropometrische Maßzahlen und Blutdruck aus der Studie zur Gesundheit von Kindern und
Jugendlichen in Deutschland (KiGGS) 2013.
Nutrition Landscape Information System (2022).
Moderate and severe thinness, underweight, overweight and obesity 2022. Available online
at https://apps.who.int/nutrition/landscape/help.aspx?menu=0&helpid=392&lang=EN(accessed
1/7/2022).
R Core Team (2021). R: A language and environment
for statistical computing. Vienna, Austria.
Scheffler, Ch./Hermanussen, M. (2021). Stunting is
the natural condition of human height. American Journal of Human Biology, e23693.
https://doi.org/10.1002/ajhb.23693.
Schüler, G. (2009). Potsdamer Längsschnittstudie
Beurteilung der körperlichen Entwicklung vom Kleinkindalter bis zum frühen Schulalter
mit Hilfe von Somatometrie, Fotogrammetrie und Morphognose. Dissertation. Potsdam,
Universität Potsdam. Available online at http://worldcatlibraries.org/wcpa/oclc/624569818.
Waterlow, J. C. (1973). Note on the assessment and
classification of protein-energy malnutrition in children. The Lancet 302 (7820), 87–89.
https://doi.org/10.1016/S0140-6736(73)93276-5.
Weissenberg, D. (1911). Das Wachstum des Menschen
nach Alter, Geschlecht und Rasse. (The growth of man according to age, sex and race):
Studien und Forschungen zur Menschen- und Völkerkunde. Stuttgart, Strecker &
Schröder.
WHO (2006). WHO Child Growth Standards -
Length/Height-for-age, Weight-for-age, Weight-for-length, Weight-for-height and Body
Mass Index-for age: Methods and Development. Geneva, World Health
Organization.
Zorlu, G. (2011). New WHO child growth standards
catch on. Bulletin of the World Health Organization 89 (4), 250–251. https://doi.org/10.2471/BLT.11.040411.