Stunting does not impair physical fitness in Indonesian school
children
Christiane Scheffler ✉
✉
Institute of Biology and Biochemistry, Human Biology, University of Potsdam,
Am Neuen Palais 10, 14467 Potsdam, Germany
Michael Hermanussen
Aschauhof, 24340 Eckernförde-Altenhof, Germany
DOI: https://doi.org/10.52905/hbph.v2.19
Abstract
Background
Physical fitness is decreased in malnourished children and adults. Poor appearance and
muscular flaccidity are among the first signs of malnutrition. Malnutrition is often
associated with stunting.
Objectives
We test the hypotheses that stunted children of low social strata are physically less
fit than children of high social strata.
Sample and Methods
We investigated 354 school girls and 369 school boys aged 5.83 to 13.83 (mean 9.54)
years from three different social strata in Kupang (West-Timor, Indonesia) in 2020. We
measured height, weight, and elbow breadth, calculated standard deviation (SDS) of
height and weight according to CDC references, and the Frame Index as an indicator of
long-term physical fitness, and we tested physical fitness in standing long jump and
hand grip strength.
Results
Children of low social strata are the physically fittest. They jump longer distances,
and they have higher values in the Frame index. No association exists between height SDS
and physical fitness, neither in respect to standing long jump, nor to hand grip
strength.
Conclusion
Stunting does not impair physical fitness in Indonesian school children. Our results
support the concept that SEPE (social-economic-political-emotional) factors are involved
in the regulation of human growth.
Keywords: stunting, standing long jump, handgrip strength, Frame Index, SEPE
Conflict of Interest: There are no
conflicts of interest.
Citation: Scheffler, C.,Hermanussen, M. (2021). Stunting does not impair physical fitness in Indonesian school
children, Human Biology and Public Health 2. https://doi.org/10.52905/hbph.v2.19.
Copyright: This is an open access article distributed under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27-07-2021 | Accepted: 18-10-2021 | Published: 22-12-2021
Take home message for students
Chronic malnutrition has characteristic clinical signs including impaired physical
fitness. Stunting is not a synonym of malnutrition. Stunted Indonesian children from low
social strata are physically fitter than the stunted children from higher social
strata.
Contents
Introduction
Physical activity is defined as any bodily movement produced by skeletal muscles that
results in energy expenditure (Westerterp 2013).
Physical activity is decreased in malnourished children and adults. Slight manifestations of
malaise, restlessness, an apparent intolerance for certain foods, a general poor appearance
and muscular flaccidity are the first signs of first degree malnutrition (Feferico Gomez, Rafael Ramos Galvan, Joaquin Cravioto and
Silvestre Frenk 1955; Behrman RE, Kliegman RM,
Jenson HB. 1999). Stunting is the result of chronic or recurrent undernutrition,
usually associated with poor socio-economic conditions, poor maternal health and nutrition,
frequent illness, and/or inappropriate infant and young child feeding and care in early life
(WHO 2021). Stunting is frequent in Indonesia.
The prevalence of stunting of children aged 5 – 12 years old was 30.7% in 2013 (Lestari et al. 2018). With a global hunger index of 22,
Indonesia is considered “seriously” affected by starvation (K. von Grebmer, J. Bernstein, N. Hossain, T. Brown, N. Prasai, Y. Yohannes, F. Patterson,
A. Sonntag, S.-M. Zimmermann, O. Towey and C. Foley. 2017).
In a recent study of stunted children in Indonesia we failed to detect the characteristic
skin lesions of malnutrition (Scheffler et al.
2021). We also failed to detect signs of malaise and restlessness, and instead, found
apparently healthy and mobile children. In order to depict the current level of physical
fitness and exclude muscular flaccidity, we decided to also study standing long jump and
hand grip strength. In order to estimate long-term activity, we measured the ratio: elbow
breadth divided by body height (Frame Index (elbow breadth to height) by Frisancho (1993) as an indicator of skeletal robusticity and
long-term level of physical activity (Rietsch et al.
2013). In view of the common perception that stunting holds children back from
reaching their physical and cognitive potential (Research
Institute, International Food Policy). We test the hypothesis that in a stunted
population of Indonesians without clinical signs of malnutrition children of lower social
strata (at higher risk of malnutrition) perform worse in tests of physical activity than
children of higher social strata (at lower risk of malnutrition), children of lower social
strata have lower values in Frame Index than children of higher social strata.
Sample and Method
We measured 723 school children, 354 girls, 369 boys aged 5.83 to 13.83 (mean 9.54) years,
from Kupang, West-Timor, Indonesia, in March 2020. These were the entire bodies of students
of two representative elementary state schools (middle social strata), situated close to the
old harbor (222 boys, 230 girls), one Catholic private school (104 boys, 92 girls) for
children of affluent parents who could afford school fees (high social strata), and one
remote run-down school outside the urban area of Kupang (43 boys, 32 girls), some 50 min
drive from the center of Kupang (low social strata). These children were impoverished and
appeared different. They were less noisy than the children from the central urban schools
were, they wore similar, but ragged and dirty school uniforms. Some had no socks or shoes.
Several had scarves or healing wounds on feet and lower leg. An additional problem in this
school seemed to be the inappropriate communication between teachers and pupils. Many
children spoke their local languages with incomplete knowledge of the national Bahasa
Indonesia. We excluded two children because of poorly healed fractures of arm and leg that
would have impaired the physical fitness test; one child refused cooperation. All
measurements were performed in the presence of the children’s teachers, and supervised and
accompanied by 26 local physicians, pediatricians, and medical residents. The group of
co-operators remained constant during the study, the variables were always obtained from the
same observers. The children were lightly dressed, and measured without shoes.
Parental informed consent was given. Parents read and sign the appropriate form that was
shown to us by the Indonesian colleagues. Ethical approval was provided by the Medical and
Health Research Ethics Committee. Faculty of Medicine, Public Health and Nursing,
Universitas Gadjah Mada-Dr, Sardjito General Hospital; Ref.NO: KE/FK 1440/EC/2019, from 11
December 2019. All individual data were anonymized.
We measured body height (technical error 2.5 mm), weight (technical error 0.15 kg), and are
looking for clinical signs of malnutrition e.g. hair, skin, and general appearance (Feferico Gomez, Rafael Ramos Galvan, Joaquin Cravioto and
Silvestre Frenk 1955). Body height was determined by digital laser rangefinder GLM
Professional® Bosch 250 VF (Schrade and Scheffler
2013) to the nearest millimeter, weight by digital scales (Soehnle, Nassau,
Germany, Style Sense Compact 100) to the nearest 100g. All measurements were taken under
standardized conditions (Knussmann 1988) as
described in detail previously (Scheffler et al.
2021). We measured hand grip strength (kPa) of the dominant hand with a vigorimeter
that was adjusted for children hand size. Each measurement consisted of two trials of which
the second was taken. And we tested the distance of long jump. As the children clustered
with much interest around the long jump group, we did not need to specifically instruct the
children. Even the youngest children were able to correctly perform the jump. Each child was
given one trial. We calculated standard deviation scores for grip strength and standing long
jump (grip_SDS, Jump_SDS). We measured elbow breadth with a caliper and calculated the Frame
index. It has previously been shown that skeletal robustness (relative elbow breadth) is
associated with daily step counts (elbow breadth/height (Frisancho 1993). High values of Frame Index indicate high physical activity over a
long time.
Standard deviation scores for height (hSDS) and weight (wSDS) were calculated according to
CDC references (Onis et al. 2007) as WHO references
do not provide data on weight above age 10 years. We also calculated SD scores for long jump
and handgrip strength for age and sex adjustment as the different groups of children were
comparably small. We compared data of different social strata with ANOVA performed scatter
plots with the R package ggplot and calculated linear mixed models using the programming
language “R” (R Core Development Team 2016).
Results
Body height standard deviation scores (hSDS) differed between social strata. Highest hSDS
(mean -0.678, SD 1.10) were found in the high social strata, medium hSDS (mean -1.271, SD
0.96) in the middle social strata, and lowest hSDS (mean -1.673, SD 0.98) in the low social
strata (p<0.001). Stunted children were found in all social strata. Body
weight was lowest in the children of the low social strata with -2.10 wSDS (SD 1.18) and
highest in the children of the high social strata with -0.42 (SD 1.64)
(p<0.001). In contrast, the children of the high social strata showed
lowest values of the Frame Index (mean 37.6, SD 2.1), the highest values (38.5, SD 1.9) was
detected in the children of the low strata (p<0.001).
Figure 1 illustrates physical performance in standing
long jump (jump_SDS). Children of the high social strata performed poorest with -0.44 SDS
(SD 0.86), children of the middle social strata showed average results with 0.14 SDS (SD
0.99), the poorest children performed best in long jump with 0.33 SDS (SD 0.96)
(p<0.001). The handgrip strength (grip_SDS) differed insignificantly
between the social strata.
Figure 1 demonstrates lack of association between
hSDS and long jump SDS (jump_sds) in any of the social strata. Figure 2 illustrates the association of height hSDS and handgrip
strength SDS (grip_SDS) (high social strata, p<0.001, adj.R²=0.14,
middle social strata p<0.001, adj.R²=0.08, low social strata
p=0.02, adj.R²=0.06). All associations are low. Very similar results were
obtained for associations between physical fitness and body weight (wSDS). Body weight
correlated low with grip strength SDS (grip_SDS) in high (p<0.001,
adj.R²=0.15), middle (p<0.001, adj.R²=0.11), and low social strata
children (p<0.001, adj.R²=0.15).
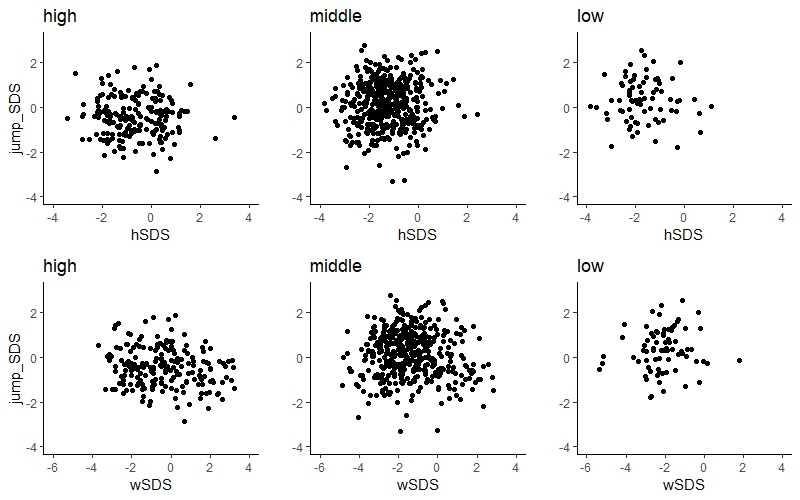
Figure 1 Association of to handgrip-strength (grip_SDS) of Indonesian primary school
children of high, middle, and low social strata (hSDS: high p<0.001,
adj.R²=0.14, middle p<0.001, adj.R²=0.08, low
p=0.02, adj.R²=0.06wSDS: high p<0.001,
adj.R²=0.15, middle p<0.001, adj.R²=0.11, low
p<0.001, adj.R²=0.15).
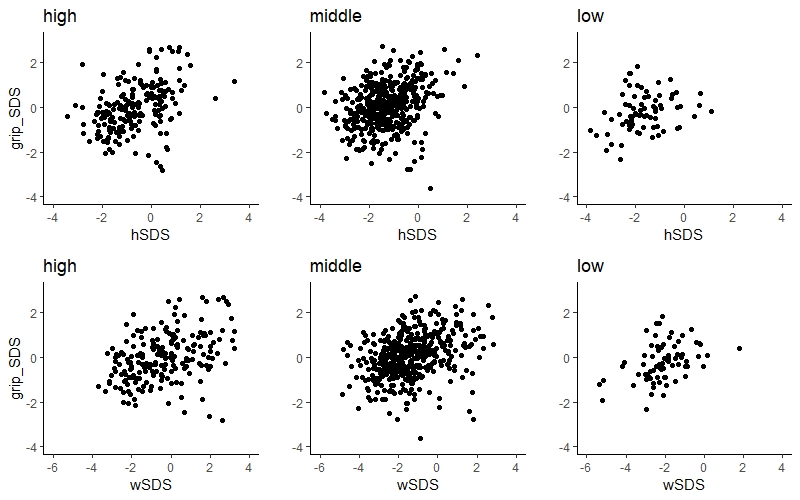
Figure 2 Association of to handgrip-strength (grip_SDS) of Indonesian primary school
children of high, middle, and low social strata (hSDS: high p<0.001,
adj.R²=0.14, middle p<0.001, adj.R²=0.08, low
p=0.02, adj.R²=0.06wSDS: high p<0.001,
adj.R²=0.15, middle p<0.001, adj.R²=0.11, low
p<0.001, adj.R²=0.15).
Discussion
Stunting (low height-for-age) is considered to result from chronic or recurrent
undernutrition, and to hold children back from reaching their physical and cognitive
potential (WHO 2021). This vision is almost
ubiquitously prevalent but has recently been questioned. Stunting is not a synonym of
malnutrition (Scheffler et al. 2019), but may
rather be considered a synonym of social disadvantage and poor parental education (Scheffler et al. 2021), and related to
socio-economic-political and emotional (SEPE) factors (Bogin 2021). In the present study, we investigated physical fitness in severely
stunted children from West Timor, Indonesia. The children originated from different social
strata, they went to school, and appeared healthy. They were physically active though to a
different extent. Particularly the children of the lowest social class showed the most
eye-catching signs of activity, with highest values of Frame Index, indicating long-term
vigorous physical exercise (Frisancho 1993; Rietsch et al. 2013) and best results in standing
long-jump, even though many of them exhibited multiple skin infections of feet and ankles as
they could not afford socks and shoes. Recent work on Frame Index of different populations
including those nutritionally at risk (Mumm et al.
2018) suggests this parameter as a relevant estimator of physical activity and
fitness.
We failed to verify the hypotheses that stunted children are physically less fit. The
effect of social disadvantage on motor development in young children has occasionally been
shown (McPhillips and Jordan-Black 2007). But though
a relatively rich literature addresses fitness of children in developing countries,
assessing a range of cultural and social factors and/or physical environmental factors in
development, these studies show inconsistent results (Barnett et al. 2016) and support the present findings. We are aware that standing
long jump and grip strength measure specific components of fitness, power and static
strength, respectively, and are not indicators of overall physical fitness. The jumping
pattern which underlies the standing long jump may be influenced by early nutritional status
and a number of the school age children may not have attained the mature movement pattern –
which will likely affect the distance jumped. Yet, neither body height, nor body weight, nor
social status and economic affluence of the parents was associated with standing long jump
and grip strength not even in children from the poorest social background. We do not deny
that caloric restriction impairs physical growth, and leads to a plethora of characteristic
clinical symptoms such as hyperchromic skin, follicular hyperkeratosis, dermatitis, muscular
flaccidity and general weakness, frequent illness, and in the long run, cognitive
restraints. However, the symptom “being shorter than given cut-offs of body height” cannot
be used as an appropriate indicator of impaired child development in the Low and Middle
Income Countries. Quite the opposite, the starting obesity epidemic in the upper social
class children of Kupang, West Timor, coincides with a decline in physical fitness
discernible by the decreased skeletal robustness and the poor performance in standing long
jump.
References
Barnett, L. M./Lai, S. K./Veldman, S. L. C./Hardy,
L. L./Cliff, D. P./Morgan, P. J./Zask, A./Lubans, D. R./Shultz, S. P./Ridgers, N.
D./Rush, E./Brown, H. L./Okely, A. D. (2016). Correlates of Gross Motor Competence in
Children and Adolescents: A Systematic Review and Meta-Analysis. Sports medicine
(Auckland, N.Z.) 46 (11), 1663–1688. https://doi.org/10.1007/s40279-016-0495-z.
Behrman, R. E./Kliegman, R. M./Jenson, H. B.
(1999). Nelson. textbook of pediatrics. 16th ed. Philadelphia, London, Toronto:
Saunders.
Bogin, B. (2021).
Social-Economic-Political-Emotional (SEPE) factors regulate human growth. Human Biology
and Public Health 1. https://doi.org/10.52905/hbph.v1.10.
Feferico Gomez, R. R. G./Joaquin, C./Silvestre, F.
(1955). Malnutrition in infancy and childhood, with special reference to Kwashiorkor.
Advances in peditarics 7, 131–169.
Frisancho, R. A. (1993). Anthropometric
standards for the assessment of growth and nutritional status. Michigan: Ann Arbor The
University of Michigan Press.
Grebmer, K. de/Bernstein, J./Hossain, N./Brown,
T./Prasai, N./Yohannes, Y./Patterson, F./Sonntag, A./Zimmermann, S.-M./Towey, O./Foley,
C. (2017). Global Hunger Index: The Inequalities of Hunger. Bonn: Welthungerhilfe;
Washington, DC: International Food Policy Research Institute; and Dublin: Concern
Worldwide.
Knussmann, R. (1988). Anthropologie: Handbuch der
vergleichenden Biologie des Menschen. Stuttgart: Fischer.
Lestari, S./Fujiati, I. I./Keumalasari, D./Daulay,
M. (2018). The prevalence and risk factors of stunting among primary school children in
North Sumatera, Indonesia. IOP Conference Series: Earth and Environmental Science 125,
12219. https://doi.org/10.1088/1755-1315/125/1/012219.
McPhillips, M./Jordan-Black, J.-A. (2007). The
effect of social disadvantage on motor development in young children: a comparative
study. Journal of Child Psychology and Psychiatry 48 (12), 1214–1222. https://doi.org/10.1111/j.1469-7610.2007.01814.x.
Mumm, R./Godina, E./Koziel, S./Musalek, M./Sedlak,
P./Wittwer-Backofen, U./Hesse, V./Dasgupta, P./Henneberg, M./Scheffler, C. (2018).
External skeletal robusticity of children and adolescents - European references from
birth to adulthood and international comparisons. Anthropologischer Anzeiger 74 (5), 383–391. https://doi.org/10.1127/anthranz/2018/0826.
Onis, M. de/Garza, C./Onyango, A. W./Borghi, E.
(2007). Comparison of the WHO child growth standards and the CDC 2000 growth charts. The
Journal of Nutrition 137 (1), 144–148. https://doi.org/10.1093/jn/137.1.144.
Research Institute, International Food Policy
(2017). 2017 global hunger index: The inequalities of hunger. Bonn: Welthungerhilfe;
Washington, DC: International Food Policy Research Institute; and Dublin: Concern
Worldwide.
Rietsch, K./Eccard, J. A./Scheffler, C. (2013).
Decreased external skeletal robustness due to reduced physical activity? American
Journal of Human Biology 25 (3), 404–410. https://doi.org/10.1002/ajhb.22389.
Scheffler, C./Hermanussen, M./Bogin, B./Liana, D.
S./Taolin, F./Cempaka, P. M. V. P./Irawan, M./Ibbibah, L. F./Mappapa, N. K./Payong, M.
K. E./Homalessy, A. V./Takalapeta, A./Apriyanti, S./Manoeroe, M. G./Dupe, F. R./Ratri,
R. R. K./Touw, S. Y./K, P. V./Murtani, B. J./Nunuhitu, R./Puspitasari, R./Riandra, I.
K./Liwan, A. S./Amandari, P./Permatasari, A. A. I./Julia, M./Batubara, J./Pulungan, A.
(2019). Stunting is not a synonym of malnutrition. European Journal of Clinical
Nutrition. https://doi.org/10.1038/s41430-019-0439-4.
Scheffler, C./Hermanussen, M./Soegianto, S. D.
P./Homalessy, A. V./Touw, S. Y./Angi, S. I./Ariyani, Q. S./Suryanto, T./Matulessy, G. K.
I./Fransiskus, T./Safira, A. V. C./Puteri, M. N./Rahmani, R./Ndaparoka, D. N./Payong, M.
K. E./Indrajati, Y. D./Purba, R. K. H./Manubulu, R. M./Julia, M./Pulungan, A. B. (2021).
Stunting as a synonym of social disadvantage and poor parental education. International
Journal of Environmental Research and Public Health 18 (3), 1350. https://doi.org/10.3390/ijerph18031350.
Schrade, L./Scheffler, C. (2013). Assessing the
applicability of the digital laser rangefinder GLM Professional Bosch 250 VF for
anthropometric field studies. Anthropologischer Anzeiger 70 (2), 137–145. https://doi.org/10.1127/0003-5548/2013/0223.
Westerterp, K. R. (2013). Physical activity and
physical activity induced energy expenditure in humans: measurement, determinants, and
effects. Frontiers in Physiology 4, 90. https://doi.org/10.3389/fphys.2013.00090.
WHO (2021). Fact sheets - malnutrition 2021.
Available online at https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed
7/26/2021).