BackgroundPreterm births not only increase the immediate morbidity and mortality of newborns but also have long-term consequences. An analysis of the risk factors is therefore of great interest from a public health perspective.
ObjectivesThe aim of this study was to analyze sex-specific differences in the association between parity and the risk of preterm birth in singleton births.
Methods6,109 female and 6,505 male neonates born at the Donaustadt Clinic in Vienna between 2010 and 2020 were included in the study. The association between sex and preterm birth in the different parity groups was analyzed using binary logistic regressions, corrected for maternal parameters and the type of conception. Within each sex, the preterm birth rates for first, third and at least fourth births were compared with those for second births (reference group).
ResultsOnly in first-born children biological sex appears to be a significant predictor of the risk of preterm birth, with biological males showing a 36.4% higher risk than biological females. When comparing within each sex, firstborn girls had a 1.844 times higher risk of preterm birth than second-born ones, and firstborn boys had a 1.740 times higher risk than second-born ones. Girls who were at least the fourth child had a 2.438 times higher risk than second-born girls.
ConclusionThere are sex-specific differences in the association between preterm birth and parity.
Keywords: parity, preterm birth, sex difference, male disadvantage
Conflict of interest statement: There are no conflicts of interest.
Citation: Nindl, S. et al. (2026). Sex differences in the association between parity and risk of preterm birth: A retrospective study from Vienna. Human Biology and Public Health. https://doi.org/10.52905/hbph2026.120.
Permissions: The copyright remains with the authors. Copyright year 2026. Unless otherwise indicated, this work is licensed under a Creative Commons License Attribution 4.0 International. This does not apply to quoted content and works based on other permissions.
According to the male disadvantage hypothesis, the rate of preterm births is significantly higher among biologically male infants. Considering the association with parity, female and male first-borns have a significantly higher risk of preterm birth compared to second-born ones. This also applies to fourth and subsequent born girls compared to second-born ones.
Contents
Introduction
Globally, the preterm birth rate in 2020 ranged from 4 to 16%, with significant regional differences. As expected, the preterm birth rate is highest in the Global South, especially in developing countries and typical low-income regions, while it is very low in the Global North and in high-income countries (WHO 2023b). In Austria in 2020, the preterm birth rate was 7.3 per 100 live births (WHO 2023a). Preterm birth is defined as a birth before the 37th week of pregnancy (WHO 2023b). Preterm birth is associated with neonatal mortality and morbidity and is the leading cause of death in children under the age of five years (Perin et al. 2022). In addition, it can lead to long-term or lifelong health problems, developmental delays, or respiratory and cardiovascular problems (Morniroli et al. 2023). An analysis of possible risk factors is therefore of great importance from a public health perspective. The etiology of preterm birth is often unknown. In addition to genetic factors and maternal illness, however, biological sex appears to play a particular role. Several studies have observed an association between preterm birth and biological male sex (Liang et al. 2024; Peelen et al. 2016; Zhang et al. 2022). On the other hand, parity, which is also associated with low birth weight and neonatal mortality, was mentioned as a risk factor (Garces et al. 2020). However, the results of various studies on the significance of parity for preterm birth are inconclusive. While many studies described higher rates among first-time mothers (Delnord et al. 2018; Kashani-Ligumsky et al. 2024; Lin et al. 2021; Prunet et al. 2017; Tracy et al. 2007), others identified higher parity as a risk factor (Esan et al. 2026; Okui and Nakashima 2025; Rugumisa et al. 2021; Zhang et al. 2022). Furthermore, the possible underlying physiological mechanisms of parity's relationship with preterm birth remain unclear.
To our knowledge, there are no studies on sex-specific differences in the relationship between parity and the risk of preterm birth, although it has been shown that maternal parameters such as suboptimal pre-pregnancy weight and low or advanced maternal age have a greater association with birth outcome and health of male newborns than on that of female newborns (Kirchengast and Hartmann 2009).
Therefore, the aim of this study is to investigate sex-typical differences in the relationship between parity and the risk of preterm birth. Two hypotheses were tested:
1.
The preterm birth rate is higher in the biological male sex than in the biological female sex.
2.
The significance of parity for preterm birth is higher in the biological male sex than in the female sex.
Data set and methods
Data set
This single-center study based on medical records included data from 12,614 single births that took place at the Clinic Donaustadt in Vienna, Austria between 2010 and 2020. Strict inclusion criteria were a single pregnancy and a live birth. Exclusion criteria were genetic abnormalities, congenital diseases, maternal diseases such as diabetes mellitus or HIV infections, and planned caesarean sections, although it should be noted that planned caesarean sections are only performed at the Clinic Donaustadt if medically indicated, not at the mother's request. A total of 6,109 female and 6,505 male newborns met the inclusion criteria. The anonymized data set was analyzed at the Department of Evolutionary Anthropology at the University of Vienna. The study was conducted in accordance with the Helsinki criteria and approved by a positive vote of the Ethics Commission of the City of Vienna (protocol number: EK 19-274-VK, 18 March 2020).
Maternal parameters
A detailed medical anamnesis of the pregnant women includes reproductive history, acute and chronic illnesses, nicotine consumption during pregnancy, and medication use. In addition, pre-pregnancy weight was reconstructed by measuring the mother's weight at the first prenatal examination, usually in the eighth gestational week, using digital scales accurate to 0.1kg. From this value and the mother's statement of her pre-pregnancy body weight, the mean value was calculated and defined as prepregnancy weight. The mother's height was also documented with a standard anthropometer during the first check-up. Body mass index (BMI) (kg/m2) was calculated to determine prepregnancy weight status. The mother's body weight was determined again before birth. The weight change during pregnancy was calculated by subtracting the prepregnancy weight from the end of pregnancy weight.
Newborn parameters
The biological sex of the newborns was determined immediately after birth. In addition, trained specialists determined the birth length of the newborns using a standard measurement board for infants and documented the birth weight using a digital infant scale.
Obstetric parameters
A birth before the 37th week of pregnancy was classified as preterm birth. The gestational age was calculated based on the first day of the last menstrual period and the results of ultrasound examinations in the first trimester. In addition, the type of conception (spontaneous or assisted) and previous pregnancies and births were documented.
Parity was divided into the following categories: parity of one (P1), parity of two (P2), parity of three (P3) and parity of four or more (Pis greater than or equal to 4). Since the parity group of two (P2) had the lowest preterm birth rate in the present sample, P2 was defined as the reference value against which the other parity values were compared, in accordance with the method by Koullali et al. (2020).
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics (version 29). Since, according to the results of the Kolmogorov-Smirnov test, no normal distribution could be assumed for maternal age, pre-pregnancy BMI, gestational weight gain, birth weight, birth length and the number of previous pregnancies, the sample parameters were given as median and semi-interquartile range. Group differences were tested for significance using the Mann-Whitney U test and Fisher's exact test.
To analyze the significance of biological sex for the association between parity and preterm birth, binary logistic regression models were created separately for each parity group with the dependent variable being the risk of preterm birth (0 corresponds to greater than or equal to 37 weeks; 1 corresponds to less than 37 weeks). We decided to perform the regression analyses for each parity group separately, because this study aimed to answer the question in which parity group sex is a significant predictor of preterm risk. To include all parity groups in one model, we would need to code parity as a dummy variable because parity is a categorical variable. In this case, we would need to define a reference group. Our analysis strategy allowed to compare the effect sizes of sex between the individual parity groups.
Sex was a predictor variable, as were maternal age (in years), pre-pregnancy BMI (in kg/m2), gestational weight gain (in kg), nicotine consumption (no=0/yes=1) and type of conception (spontaneous=0/assisted=1). After Bonferroni correction, the new significance level here was p is less than 0.0125.
For the comparison within the biological sex, a binary logistic regression model for each sex was performed with the dependent variable risk of preterm birth (0 corresponds to greater than or equal to 37 weeks; 1 corresponds to 1 equals is less than 37 weeks). Parity was coded as a dummy variable with a parity of two as the reference. Parities of 1, 3, and at least 4 – each compared to parity of 2 – were predictor variables, as well as maternal age, pre-pregnancy BMI, gestational weight gain, nicotine consumption and type of conception.
Results
Table 1 shows the maternal and neonatal parameters as well as the obstetric characteristics separated by sex. Significant differences between the two sexes existed only in birth weight and birth length, as well as in the preterm birth rate. Male newborns were significantly longer and heavier, but more likely to be born preterm. Their preterm birth rate (6.1%; n=396) was significantly higher than in female newborns (4.9%; n=299). The risk of being born preterm was 26% higher in the male sex (chi squared equals 8.615, p equals 0.003).
Table 1 Maternal, newborn and obstetrical characteristics according to sex
females
males
n
Median
SIQR
range
Median
SIQR
range
p-value
Maternal age (yrs)
31
3.5
14-55
30
3.5
15-54
0.412
PPBMI (kg/m2)
22.86
2.85
13.30-58.09
22.86
2.86
14.13-57.30
0.957
Body height (cm)
165
5.0
141-188
165
4.5
140-193
0.753
Weight gain (kg)
14
3.5
-17 - 43
14
4.0
-17 - 41
0.120
Birth weight (g)
3340
295
470-5809
3500
320
700-5350
<0.001*
Birth length (cm)
50
1.5
28-60
51
1.5
33-58
<0.001*
Gestational week
39
0.5
26-42
39
1.0
26-42
0.243
Pregnancies
2
1.0
1-14
2
1.0
1-15
0.397
Previous births
2
0.5
1-9
2
0.5
1-10
0.175
n
%
n
%
Preterm birth
299
4.9%
396
6.1%
<0.001*
Parity 1 (P1)
2851
46.7%
2964
45.6%
0.594
Parity 2 (P2)
2191
35.9%
2361
36.3%
Parity 3 (P3)
733
12.0%
818
12.6%
Parity is greater than or equal to 4 (Pis greater than or equal to 4)
334
5.5%
362
5.6%
ART
186
3.0%
169
2.6%
0.072
Nicotine
854
14%
857
13.2%
0.098
Legend: PPBMI = prepregnancy body mass index ; ART = Artificial reproductive technology
SIQR=semi-interquartile range, P1=primi-parity, P2=parity score of two, P3=parity score of three, Pis greater than or equal to 4=parity score of at least four
significance level=p<0.05; significant results are asterisked (*)
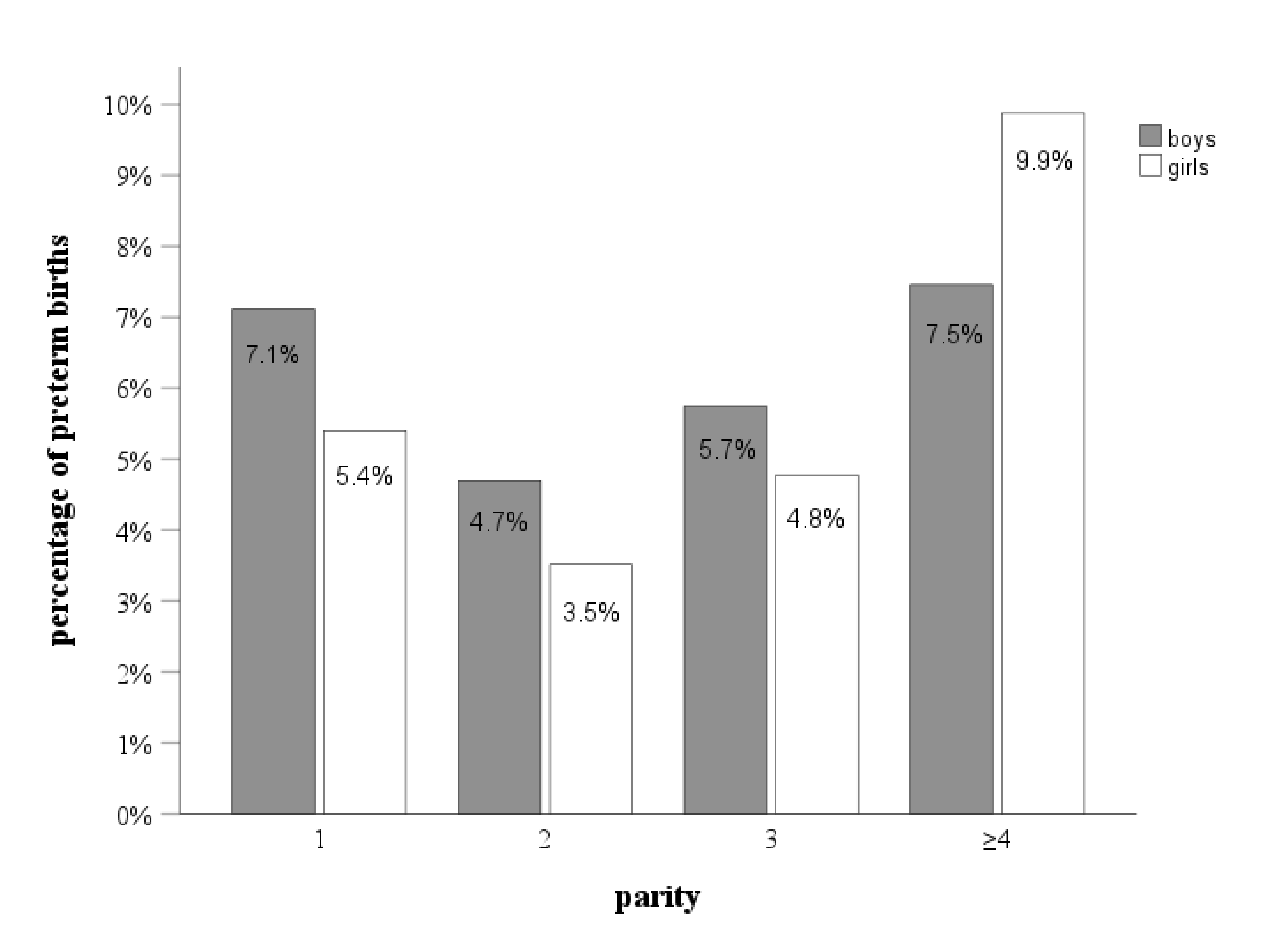
Figure 1 Percentage of preterm deliveries in each parity group separated by sex. Sample size in each parity group: parity 1: nboys=2964, ngirls=2851; parity 2: nboys=2361, ngirls=2191; parity 3: nboys=818, ngirls=733; parity ≥4: nboys=362, ngirls=334 Absolute frequencies of preterm birth: parity 1: nboys=211, ngirls=154; parity 2: nboys=111, ngirls=77; parity 3: nboys=47, ngirls=35; parity ≥4: nboys=27, ngirls=33
Figure 1 shows the percentages of preterm births in each parity group, separated by sex. Males showed an approximately U-shaped distribution, while female newborns showed a more J-shaped one.
Table 2 presents the associations between sex and risk of preterm birth within each parity group. All models, except that of Pis greater than or equal to 4, were statistically significant (p(P1) < 0.001; p(P2) < 0.001; p(P3)=0.008; p(Pis greater than or equal to 4) = 0.136), Nagelkerke R2 was 0.030, 0.047, 0.033, and 0.031 respectively. Sex was significantly associated with preterm birth in first-borns. Male first-borns had a 36.4% higher risk of being born preterm than female first-borns. Second-born boys had a 40.9% higher risk of being born preterm than their female counterparts, but this association was no longer significant after Bonferroni correction. Other significant predictors of preterm birth are maternal weight gain in first-, second-, and third-borns as well as maternal age and nicotine consumption in first- and second-born children.
Table 2 Sex and risk of preterm birth within each parity group
Parity
95%-CI of Exp(B)
B
Exp(B)
lower value
upper value
p
P1
Sex
0.310
1.364
1.099
1.692
0.005*
Maternal age (yrs)
0.026
1.026
1.006
1.047
0.009*
PPBMI (kg/m2)
0.003
1.003
0.982
1.025
0.759
Weight gain (kg)
-0.060
0.942
0.924
0.961
<0.001*
ART
0.415
1.514
0.982
2.334
0.060
Nicotine
0.435
1.545
1.149
2.077
0.004*
P2
Sex
0.343
1.409
1.044
1.900
0.025
Maternal age (yrs)
0.045
1.046
1.016
1.077
0.003*
PPBMI (kg/m2)
-0.021
0.979
0.949
1.009
0.166
Weight gain (kg)
-0.091
0.913
0.887
0.941
<0.001*
ART
-0.694
0.500
0.121
2.067
0.338
Nicotine
0.837
2.310
1.579
3.380
<0.001*
P3
Sex
0.219
1.245
0.792
1.957
0.342
Maternal age (yrs)
0.030
1.030
0.985
1.078
0.193
PPBMI (kg/m2)
-0.064
0.938
0.891
0.988
0.015
Weight gain (kg)
-0.076
0.927
0.887
0.968
0.001*
ART
-18.513
0.000
0.000
.
0.999
Nicotine
-0.106
0.900
0.484
1.671
0.738
P≥4
Sex
-0.313
0.731
0.427
1.250
0.252
Maternal age (yrs)
-0.031
0.969
0.916
1.025
0.272
PPBMI (kg/m2)
0.008
1.008
0.959
1.059
0.751
Weight gain (kg)
-0.043
0.958
0.914
1.005
0.080
ART
-18.666
0.000
0.000
.
0.999
Nicotine
0.516
1.675
0.915
3.067
0.094
Legend: PPBMI = prepregnancy body mass index ; ART = Artificial reproductive technology
P1=primiparity, P2=parity score of two, P3=parity score of three, Pis greater than or equal to 4=parity score of at least four
sex coded 0=female newborns, 1=male newborns
significance level=p<0.0125; significant results are asterisked (*)
The association between parity and the risk of preterm birth for each sex is shown in Table 3. The models for both boys and girls were statistically significant (p<0.001), Nagelkerke R2 was 0.038 and 0.035 respectively. Compared to the second-born, the first-born child had a significantly increased risk of being preterm. First-born girls had a 1.844 times higher risk of being born preterm than second-born children of the same sex, and first-born boys had a 1.740 times higher risk. The risk of preterm birth did not differ significantly between third-born and second-born children. This applied to both biological sexes. The risk of preterm birth for at least fourth-born boys also did not differ significantly from that for second-born boys. Fourth-born girls, on the other hand, had a significantly 2.438 times higher risk of preterm birth. In both girls and boys other significant predictors for preterm birth were maternal age, gestational weight gain and nicotine consumption.
Table 3 Parity and risk of preterm birth
95%-CI of Exp(B)
B
Exp(B)
lower value
upper value
p
Preterm birth risk in boys
P1 vs. P2
0.554
1.740
1.363
2.221
<0.001*
P3 vs. P2
0.119
1.126
0.789
1.608
0.514
P≥4 vs. P2
0.298
1.347
0.858
2.115
0.195
Maternal age (yrs)
0.022
1.022
1.002
1.043
0.028*
PPBMI (kg/m2)
-0.021
0.980
0.959
1.001
0.057
Weight gain (kg)
-0.073
0.930
0.912
0.948
<0.001*
ART
0.402
1.495
0.889
2.515
0.129
Nicotine
0.591
1.805
1.380
2.361
<0.001*
Preterm birth risk in girls
P1 vs. P2
0.612
1.844
1.385
2.456
<0.001*
P3 vs. P2
0.227
1.255
0.831
1.896
0.281
Pis greater than or equal to 4 vs. P2
0.891
2.438
1.570
3.784
<0.001*
Maternal age (yrs)
0.033
1.034
1.011
1.057
0.004*
PPBMI (kg/m2)
0.005
1.005
0.981
1.029
0.701
Weight gain (kg)
-0.058
0.943
0.923
0.964
<0.001*
ART
0.039
1.040
0.547
1.977
0.905
Nicotine
0.366
1.442
1.050
1.980
0.024*
Legend: PPBMI = prepregnancy body mass index ; ART = Artificial reproductive technology
P1=parity of one (coded 1) compared to parity of two (coded 0), P3=parity of three (coded 1)
compared to parity of two (coded 0), Pis greater than or equal to 4=parity of at least 4 (coded 1) compared to parity of two (coded 0)
significant results are asterisked (*)
In general, it should be noted, that statistical power especially in parity group Pis greater than or equal to 4 is limited due to small sample size, which is why results should be interpreted with caution.
Discussion
In our study, we found a marked impact of sex on preterm birth rate, but also on the association between parity and preterm birth. The first hypothesis, that preterm birth is more common in the biological male sex than in the biological female sex, was verified in this study. It corresponds to the results of other studies (Liang et al. 2024; Peelen et al. 2016; Zhang et al. 2022) and can be interpreted in terms of the male disadvantage hypothesis. This hypothesis refers to sex differences in intrauterine as well as postnatal morbidity and mortality with a male disadvantage and the higher susceptibility of male fetuses to stress factors and suboptimal maternal conditions which is well reported by several studies (e.g., Elsmén et al. 2004; Kirchengast and Hartmann 2009; Mondal et al. 2014; Qiu et al. 2020). What causes this sex differences is yet unknown. In a review, Clifton (2010) suggested that differences in the structure and function of the placenta as well as different fetal-placental patterns of gene and protein expression, immune function, steroid profile and growth factor pathway could play a role.
The second hypothesis presented in the introduction, that parity has a greater influence on preterm birth in the biological male sex, could not be clearly verified. First-born boys had a significantly higher risk of 36.4% of being born preterm than first-born girls, which represents a disadvantage for boys. Second-born boys also appeared to have a higher risk (approximately 40.9% higher) than second-born girls, although this was not significant after correction for multiple tests. So far, hypothesis 2 would be confirmed.
Being the first-born child was a significant risk factor for preterm birth for both biological sexes compared to the second-born ones of the corresponding sex. Apparently, there was a slightly stronger association in girls. Female first-borns had a 1.844 times higher risk of preterm birth, while male firstborns had a slightly lower risk (1.740 times higher risk). In addition, parity of at least four was a risk factor for preterm birth only in female newborns compared to parity of two.
As mentioned above, there are many studies that consider first birth to be a risk factor, but some studies have also found that higher parity is associated with an increased risk of preterm birth. Hu et al. (2018) observed an increased risk of preterm birth in women with a parity of is greater than or equal to 4. Koullali et al. (2020) showed that women have an increased risk of preterm birth during their first and fifth pregnancies, while Meis et al. (1995) report a U-shaped relationship between parity and the risk of preterm birth. In the present study, this applies to the biological male sex, while a more J-shaped association was observed in the biological female sex (Figure 1).
First births and a high number of births are risk factors in our study. This is not surprising: the first birth presents new challenges for the mother's body, while a high number of births places particular strain on the mother's body.
The direct mechanisms are not yet clear. Some parameters associated with the risk of preterm birth have also been found to be associated with parity. These include behavioral differences, such as increased fear of childbirth among first-time mothers (Rouhe et al. 2009) and women whose first birth was preterm, who are more likely to refrain from a second pregnancy (Miranda et al. 2011). The frequency of prenatal care visits among multiparous women (Otieku et al. 2021) could play an important role in the relationship between parity and the risk of preterm birth. In addition, some physiological phenomena have been postulated that are associated with both parity and preterm birth. Primiparity as a risk factor could, for example, be due to more sensitive membranes, leading to a higher incidence of premature membrane rupture (Robin et al. 2024), a smaller uterine cavity and reduced uteroplacental blood flow (Lin et al. 2021) or higher ferritin concentrations (Broekhuis et al. 2024). Higher parity could increase the risk of preterm birth due to lower hemoglobin concentrations (Ali et al. 2020), maternal anemia (Liabsuetrakul 2011; Kumari et al. 2019), a higher incidence of certain medical complications and placental pathologies (Aliyu et al. 2005) and uterine changes due to previous pregnancies (Wagura et al. 2018). In general, the vaginal microbiome is altered by parity, which could be associated with adverse pregnancy outcomes (Kashani-Ligumsky et al. 2024).
In accordance with other studies reporting increased vulnerability in males in connection with suboptimal maternal conditions and parameters (Kirchengast and Hartmann 2009), this study also showed that male sex is a significant predictor of the risk of preterm birth in first-born children and possibly also in second-born children. However, when comparing within the same sex, newborns who were at least the fourth child had a significantly higher risk of preterm birth than second-born children only in girls.
Two explanations are proposed for the different patterns of association between the risk of preterm birth and parity between and within sexes. Firstly, it is possible that in groups with higher parity, such as groups P3 and Pis greater than or equal to 4, the association of parity with the risk of preterm birth becomes even stronger in females. Accordingly, no significant sex difference could be observed in these parity groups. Furthermore, in the Pis greater than or equal to 4 group, there appears to be a tendency for girls to be at higher risk, although this is not statistically significant. This could possibly be due to the small sample size in this group. It could therefore even be the case that in groups with higher parity, such as Pis greater than or equal to 4, the risk in females exceeds that in males. Male newborns had a higher percentage of preterm births than females in every parity group, except in the Pis greater than or equal to 4 group. Here, the incidence was 7.5% for boys and 9.9% for girls. Furthermore, only in the Pis greater than or equal to 4 group was there a negative correlation between sex and the risk of preterm birth, albeit not a significant one – again, possibly due to the small sample size in this group. This initial explanation would suggest that in groups with low parity there is a disadvantage for males, but in groups with higher parity there is a disadvantage for females.
In contrast, the second explanation, would refer to a male disadvantage also in the higher parity groups resulting in a higher intrauterine mortality. Studies suggest that high parity is associated with a significantly increased risk of stillbirth (Awoleke and Adanikin 2016; Dasa et al. 2022). Accordingly, it is possible that an adverse impact of parity in first-born boys would result in an increased risk in preterm birth but in higher parity groups it would lead to higher intrauterine mortality. Thus, females would survive more likely but would show consequences not in form of higher intrauterine mortality but of increased preterm birth incidence.
This study has several limitations. It is a single-center study, so the results may not be transferable to other regions or population groups. As it was a retrospective study, it was not possible to control for other factors that influence the risk of preterm birth. No information was available on socioeconomic status or previous preterm births among siblings, which are known risk factors for preterm birth. In addition, the sample size in the groups with higher parity – especially Pis greater than or equal to 4 – was rather small, which may limit the possibilities for interpretation.
Conclusion
Future studies should focus not only on elucidating the mechanisms behind the relationship of parity with preterm birth, but also on the mechanisms behind the sex differences observed here. As this study is the first to examine sex differences in the association between preterm birth and parity, it needs to be replicated, particularly in countries with high fertility rates. This could be clinically significant not only for preventive measures, but also for the interpretation of data from countries where higher birth rates are more common and sex differences in neonatal mortality are reported.
Funding statement
There was no funding.
References
Ali, S. A./Tikmani, S. S./Saleem, S./Patel, A. B./Hibberd, P. L./Goudar, S. S./Dhaded, S./Derman, R. J./Moore, J. L./McClure, E. M./Goldenberg, R. L. (2020). Hemoglobin concentrations and adverse birth outcomes in South Asian pregnant women: findings from a prospective Maternal and Neonatal Health Registry. Reproductive Health 17 (Suppl 2), 154. https://doi.org/10.1186/s12978-020-01006-6.
Awoleke, J. O./Adanikin, A. I. (2016). Baird-Pattinson Aetiological Classification and Phases of Delay Contributing to Stillbirths in a Nigerian Tertiary Hospital. Journal of pregnancy 2016, 1703809. https://doi.org/10.1155/2016/1703809.
Broekhuis, A./Koenen, S. V./Broeren, M. A. C./Krabbe, J. G./Pop, V. J. M. (2024). High first trimester ferritin levels differ according to parity and are independently related to preterm birth: A prospective cohort study. Acta Obstetricia et Gynecologica Scandinavica 103 (7), 1437–1443. https://doi.org/10.1111/aogs.14830.
Dasa, T. T./Okunlola, M. A./Dessie, Y. (2022). Effect of Grand Multiparity on the Adverse Birth Outcome: A Hospital-Based Prospective Cohort Study in Sidama Region, Ethiopia. International journal of women's health 14, 363–372. https://doi.org/10.2147/IJWH.S350991.
Delnord, M./Blondel, B./Prunet, C./Zeitlin, J. (2018). Are risk factors for preterm and early-term live singleton birth the same? A population-based study in France. BMJ open 8 (1), e018745. https://doi.org/10.1136/bmjopen-2017-018745.
Elsmén, E./Steen, M./Hellström-Westas, L. (2004). Sex and gender differences in newborn infants: why are boys at increased risk? The Journal of Men's Health & Gender 1 (4), 303–311. https://doi.org/10.1016/j.jmhg.2004.09.010.
Esan, D. T./Alivide, D. S./Nmamdi, B. P./Olajide, A. O./Ogunmuyiwa, A. O./Oyama, B. O./Samson, T. K./Ramos, C. G. (2026). Prevalence and neonatal morbidities associated with preterm birth: A three-year retrospective study at Ekiti State University Teaching Hospital, Nigeria. Global Pediatrics 15, 100319. https://doi.org/10.1016/j.gpeds.2026.100319.
Garces, A./Perez, W./Harrison, M. S./Hwang, K. S./Nolen, T. L./Goldenberg, R. L./Patel, A. B./Hibberd, P. L./Lokangaka, A./Tshefu, A./Saleem, S./Goudar, S. S./Derman, R. J./Patterson, J./Koso-Thomas, M./McClure, E. M./Krebs, N. F./Hambidge, K. M. (2020). Association of parity with birthweight and neonatal death in five sites: The Global Network’s Maternal Newborn Health Registry study. Reproductive Health 17 (Suppl 3), 182.
Hu, C.-Y./Li, F.-L./Jiang, W./Hua, X.-G./Zhang, X.-J. (2018). Pre-Pregnancy Health Status and Risk of Preterm Birth: A Large, Chinese, Rural, Population-Based Study. Medical Science Monitor 24, 4718–4727. https://doi.org/10.12659/MSM.908548.
Kashani-Ligumsky, L./Neiger, R./Segal, E./Cohen, R./Lopian, M. (2024). Is Parity a Risk Factor for Late Preterm Birth? Results from a Large Cohort Study. Journal of Clinical Medicine 13 (2). https://doi.org/10.3390/jcm13020429.
Kirchengast, S./Hartmann, B. (2009). The Male Disadvantage Hypothesis Reconsidered: Is There Really a Weaker Sex? An Analysis of Gender Differences in Newborn Somatometrics and Vital Parameters. Journal of Life Sciences 1 (1), 63–71. https://doi.org/10.1080/09751270.2009.11885136.
Koullali, B./van Zijl, M. D./Kazemier, B. M./Oudijk, M. A./Mol, B. W. J./Pajkrt, E./Ravelli, A. C. J. (2020). The association between parity and spontaneous preterm birth: a population based study. BMC Pregnancy and Childbirth 20 (1), 233–248. https://doi.org/10.1186/s12884-020-02940-w.
Kumari, S./Garg, N./Kumar, A./Guru, P. K. I./Ansari, S./Anwar, S./Singh, K. P./Kumari, P./Mishra, P. K./Gupta, B. K./Nehar, S./Sharma, A. K./Raziuddin, M./Sohail, M. (2019). Maternal and severe anaemia in delivering women is associated with risk of preterm and low birth weight: A cross sectional study from Jharkhand, India. One Health 8, 100098. https://doi.org/10.1016/j.onehlt.2019.100098.
Liabsuetrakul, T. (2011). Is international or Asian criteria-based body mass index associated with maternal anaemia, low birthweight, and preterm births among Thai population? An observational study. Journal of Health, Population, and Nutrition 29 (3), 218–228. https://doi.org/10.3329/jhpn.v29i3.7869.
Liang, X./Lyu, Y./Li, J./Li, Y./Chi, C. (2024). Global, regional, and national burden of preterm birth, 1990-2021: a systematic analysis from the global burden of disease study 2021. E Clinical Medicine 76, 102840. https://doi.org/10.1016/j.eclinm.2024.102840.
Lin, L./Lu, C./Chen, W./Li, C./Guo, V. Y. (2021). Parity and the risks of adverse birth outcomes: a retrospective study among Chinese. BMC Pregnancy and Childbirth 21 (1), 257. https://doi.org/10.1186/s12884-021-03718-4.
Meis, P. J./Michielutte, R./Peters, T. J./Wells, H. B./Sands, R. E./Coles, E. C./Johns, K. A. (1995). Factors associated with preterm birth in Cardiff, Wales. I. Univariable and multivariable analysis. American Journal of Obstetrics and Gynecology 173 (2), 590–596. https://doi.org/10.1016/0002-9378(95)90287-2.
Miranda, M. L./Edwards, S. E./Myers, E. R. (2011). Adverse birth outcomes among nulliparous vs. multiparous women. Public Health Reports 126 (6), 797–805. https://doi.org/10.1177/003335491112600605.
Mondal, D./Galloway, T. S./Bailey, T. C./Mathews, F. (2014). Elevated risk of stillbirth in males: systematic review and meta-analysis of more than 30 million births. BMC medicine 12, 220. https://doi.org/10.1186/s12916-014-0220-4.
Morniroli, D./Tiraferri, V./Maiocco, G./Rose, D. U. de/Cresi, F./Coscia, A./Mosca, F./Giannì, M. L. (2023). Beyond survival: the lasting effects of premature birth. Frontiers in Pediatrics 11, 1213243. https://doi.org/10.3389/fped.2023.1213243.
Okui, T./Nakashima, N. (2025). Association of grand multiparity with adverse birth outcomes and sociodemographic characteristics: an analysis of nationwide birth data in Japan. Reproductive Health 23 (1), 26. https://doi.org/10.1186/s12978-025-02246-0.
Otieku, E./Fenny, A./Labi, A.-K./Enemark, U. (2021). Incidence of preterm births in a referral teaching hospital in Ghana: What is the role of maternal age, parity, gravidity and stress during pregnancy? South African Journal of Child Health 15 (3), 154–158. https://doi.org/10.7196/SAJCH.2021.V15I3.01777.
Peelen, M. J. C. S./Kazemier, B. M./Ravelli, A. C. J./Groot, C. J. M. de/van der Post, J. A. M./Mol, B. W. J./Hajenius, P. J./Kok, M. (2016). Impact of fetal gender on the risk of preterm birth, a national cohort study. Acta Obstetricia et Gynecologica Scandinavica 95 (9), 1034–1041. https://doi.org/10.1111/aogs.12929.
Perin, J./Mulick, A./Yeung, D./Villavicencio, F./Lopez, G./Strong, K. L./Prieto-Merino, D./Cousens, S./Black, R. E./Liu, L. (2022). Global, regional, and national causes of under-5 mortality in 2000–19: an updated systematic analysis with implications for the Sustainable Development Goals. The Lancet Child & Adolescent Health 6 (2), 106–115. https://doi.org/10.1016/S2352-4642(21)00311-4.
Prunet, C./Delnord, M./Saurel-Cubizolles, M.-J./Goffinet, F./Blondel, B. (2017). Risk factors of preterm birth in France in 2010 and changes since 1995: Results from the French National Perinatal Surveys. Journal of gynecology obstetrics and human reproduction 46 (1), 19–28. https://doi.org/10.1016/j.jgyn.2016.02.010.
Qiu, X./Fong, K. C./Shi, L./Papatheodorou, S./Di, Q./Just, A./Kosheleva, A./Messerlian, C./Schwartz, J. D. (2020). Prenatal exposure to particulate air pollution and gestational age at delivery in Massachusetts neonates 2001-2015: A perspective of causal modeling and health disparities. Environmental epidemiology (Philadelphia, Pa.) 4 (5), e113. https://doi.org/10.1097/EE9.0000000000000113.
Robin, A./Tessier Doyen, N./Ben Rhaiem, S./Valette, N./Fermeaux, V./Preux, P.-M./Martinez, S./Eyraud, J.-L./El Hamel, C./Riethmuller, D./Coste Mazeau, P. (2024). Influence of clinical risk factors for preterm premature rupture of membranes (PPROM) on the elastic strength of fetal membranes at term: A prospective study. PloS One 19 (12), e0312760. https://doi.org/10.1371/journal.pone.0312760.
Rouhe, H./Salmela-Aro, K./Halmesmäki, E./Saisto, T. (2009). Fear of childbirth according to parity, gestational age, and obstetric history. BJOG : An International Journal of Obstetrics and Gynaecology 116 (1), 67–73. https://doi.org/10.1111/j.1471-0528.2008.02002.x.
Rugumisa, B. T./Bongcam‐Rudloff, E./Lukumay, M. S./Lyantagaye, S. L. (2021). Factors associated with risk of preterm delivery in Tanzania: A case‐control study at Muhimbili National Hospital. International Journal of Gynecology & Obstetrics 154 (2), 318–323. https://doi.org/10.1002/ijgo.13520.
Tracy, S. K./Tracy, M. B./Dean, J./Laws, P./Sullivan, E. (2007). Spontaneous preterm birth of liveborn infants in women at low risk in Australia over 10 years: a population-based study. BJOG : An International Journal of Obstetrics and Gynaecology 114 (6), 731–735. https://doi.org/10.1111/j.1471-0528.2007.01323.x.
Wagura, P./Wasunna, A./Laving, A./Wamalwa, D./Ng'ang'a, P. (2018). Prevalence and factors associated with preterm birth at kenyatta national hospital. BMC Pregnancy and Childbirth 18 (1), 107. https://doi.org/10.1186/s12884-018-1740-2.
 ✉
✉