BackgroundResearch increasingly suggests that vitamin D plays a significant role in the development and severity of allergic diseases. However, less is known about how vitamin D status and allergic sensitization may jointly influence bone health.
ObjectiveThe aim of this study was to investigate the relationship between allergies, vitamin D levels and bone quality and quantity in a Slovak adult population.
Sample and Methods
The sample consisted of 198 participants aged 19–57, 53 men with a mean age of 36.6±9.6 years (16 without allergy, 37 with allergy) and 145 women with a mean age of 36.1±10.0 years (48 without allergy, 97 with allergy). Allergy diagnosis was confirmed by a physician in an immunoallergology outpatient clinic. Health data (medical history, lifestyle, allergy history/treatment and vitamin supplementation) were collected by questionnaire and bone tissue quality and quantity parameter (T-score, Z-score) were assessed using a Sunlight MiniOmni ultrasound densitometer.
ResultsAmong women, Mann–Whitney U tests showed lower vitamin D with grass (p=0.006; rrb=0.375) and animal allergy (p=0.011; rrb=0.453). Moreover, in t tests, Z-scores were lower in women with animal allergy (p=0.047; 0.26 vs 0.76). Among men, animal allergy was associated with reduced T- and Z-scores (p=0.035 for both) and showed negative correlations with T-score (p=0.035; r=−0.297) and Z-score (p=0.035; r=−0.296).
ConclusionsSpecific allergic conditions may be associated with lower vitamin D levels and reduced bone tissue quality and quantity, with notable sex-specific patterns.
Keywords: bone quality, bone quantity, vitamin D, allergic diseases, Slovak adult population
Citation: Hozáková, A. et al. (2026). Allergy is associated with bone quality and quantity. Human Biology and Public Health. https://doi.org/10.52905/hbph2026.114.
Permissions: The copyright remains with the authors. Copyright year 2026. Unless otherwise indicated, this work is licensed under a Creative Commons License Attribution 4.0 International. This does not apply to quoted content and works based on other permissions.
Allergies in Slovak adults were linked to lower vitamin D and reductions in bone tissue quality and quantity, with sex-specific patterns. Although these findings reflect correlations rather than causation, they suggest that early attention to vitamin D and bone health in allergic patients may help prevention.
Contents
Introduction
Allergic diseases arise from an exaggerated immune response to allergens, mediated by a wide range of immune cells, including lymphocytes, mast cells and basophils, as well as immune molecules such as immunoglobulin E (IgE) (Zhang et al. 2024). These conditions, which include allergic rhinitis, asthma, atopic dermatitis, food allergy and eczema, develop through multifactorial mechanisms involving both genetic predisposition and environmental exposures (Wang et al. 2023). Increasing evidence suggests that vitamin D may influence these immune pathways, as low vitamin D status has been linked with higher markers of atopy and greater prevalence of allergic diseases (Douros et al. 2015; Özdemir 2016).
Vitamin D is a secosteroid hormone with a fundamental role in calcium absorption and the regulation of calcium and phosphate homeostasis. Through these mechanisms, it contributes critically to bone mineralization and is positively associated with bone mineral density (BMD) (Bora et al. 2018; Laird et al. 2010).
The relationship between vitamin D status and allergic diseases has been widely investigated; several studies report significantly higher prevalence of vitamin D deficiency among individuals with allergic conditions than among healthy controls (Lipińska-Opałka et al. 2021; Ma et al. 2020). However, not all studies have confirmed these associations, and the evidence regarding the role of vitamin D in allergic diseases remains partly inconsistent, which highlights the need for further investigation (Lombardi et al. 2017; Rueter et al. 2022).
In addition to these immunological effects, vitamin D remains a key regulator of bone tissue health. Vitamin D facilitates the absorption of calcium in the intestine and contributes to maintaining adequate serum calcium concentrations, which are essential for proper bone mineralization (Martinis et al. 2020). It also plays an active role in bone growth and remodelling by regulating the activity of osteoblasts and osteoclasts (Bouillon et al. 2019). Deficiency of vitamin D disrupts these processes, leading to accelerated bone turnover, loss of bone mass and an increased risk of osteoporotic fractures (Martinis et al. 2021; Hewison 2012).
Beyond the well-established roles of vitamin D, recent findings suggest that bone metabolism may also be affected indirectly by mechanisms linked to allergic diseases. The activation of mast cells and eosinophils during allergic reactions leads to the release of inflammatory mediators such as histamine, tryptase and cytokines, which contribute to systemic inflammation (Murdaca et al. 2022; Ponzetti and Rucci 2019). Chronic inflammation of this type can disturb the balance between bone formation and resorption, promoting osteoclast activity over osteoblast function and ultimately reducing BMD (Jung et al. 2014; Sirufo et al. 2020). Clinical evidence further supports the link between allergic diseases and impaired bone health. Patients with atopic dermatitis had an increased risk of fractures even in the absence of corticosteroid use, with the risk being highest in severe disease (Wu et al. 2017a). Similarly, (Choi and Kong 2019) reported a higher prevalence of osteoporosis among patients with chronic rhinosinusitis. Research focusing on children with food allergies, particularly those allergic to cow’s milk protein or multiple food items, have also shown an increased risk of vitamin D deficiency, osteopenia and impaired bone metabolism (Doulgeraki et al. 2017). These findings suggest that allergic diseases themselves may contribute to impaired bone quality and quantity.
Despite accumulating evidence of interactions between vitamin D, allergic inflammation and bone metabolism, the relationship remains insufficiently clarified. Previous studies have demonstrated that allergic diseases such as atopic dermatitis, chronic rhinosinusitis and food allergies may increase the risk of reduced BMD and osteoporosis (Choi and Kong 2019; Doulgeraki et al. 2017; Wu et al. 2017b). However, the overall findings are inconsistent, with some reports supporting significant associations and others failing to confirm a direct link. Yet, the extent to which vitamin D deficiency and allergic sensitisation jointly affect bone quality and quantity has not been fully elucidated. To address this gap, our study aimed to investigate the associations between allergies, vitamin D levels and bone tissue parameters in a Slovak adult population. We hypothesised that individuals with allergies would have lower bone tissue quality and quantity than those without allergies and individuals with allergies would have significantly lower vitamin D levels than non-allergic individuals.
Sample and methods
This study was conducted at an immunoallergology outpatient clinic in Bratislava, Slovakia, and data were collected from February to December 2024.
Sample
We enrolled 198 adults aged 19–57 years, born between 1967 and 2005: 53 men (mean age 36.6±9.6 years; 16 without allergy, 37 with allergy) and 145 women (mean age 36.1±10.0 years; 48 without allergy, 97 with allergy). No exclusion criteria were applied. Comorbid conditions (e.g., oncologic and endocrine disorders and inflammatory bowel disease) were recorded. In exploratory analyses, these conditions did not show statistically significant correlations with bone parameters (T-score and Z-score), so all participants were retained for analysis. The study protocol was approved by the Ethics Committee of Comenius University in Bratislava (approval Number: ECH19040). All participants provided written informed consent in accordance with the Declaration of Helsinki (2013 revision).
Allergy diagnosis
Allergy diagnoses were established by a physician based on clinical examination in the immunoallergology clinic. Health information was compiled from outpatient medical records, a structured questionnaire and an in-person interview. The questionnaire covered medical history, lifestyle, allergy history and intake of vitamins and other supplements. Participants were classified into the following allergy categories: food, dust mites, pollen, grasses, animal and skin allergies.
Anthropometry
Trained personnel measured standing height and body weight following standardised anthropometric procedures (Lohman et al. 1988). Height was recorded to the nearest 0.5 cm using a Siber & Hegner anthropometer, with participants upright, heels together, back against the wall. Body weight was measured with a Luxa 3 scale. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m²).
Dietary supplements
Dietary supplement use was assessed using an open-ended questionnaire item (“Which dietary supplements do you take?”). In addition, participants answered specific yes/no questions on vitamin D and calcium supplementation. Based on these responses, we identified supplementation with vitamin D, calcium, vitamin C, B vitamins, magnesium, zinc and multivitamin complexes.
Vitamin D
Venous blood was drawn on site by a trained nurse at the immunoallergology clinic and submitted to an accredited clinical biochemistry laboratory for analysis. Total vitamin D concentrations were quantified according to the laboratory’s standard procedures and reported in nmol/l. The reference range for total vitamin D was 75.0–100.0nmol/l.
Assessment of bone quality and quantity
Bone parameters were assessed using quantitative ultrasonography (QUS; Sunlight MiniOmni™, BeamMed, Israel), a non-invasive device that evaluates bone quality and quantity by determining the speed of sound (SOS; m/s) through bone tissue. Higher SOS values reflect greater bone density and are influenced by cortical thickness, bone microstructure and elasticity, as ultrasound waves interact with bone differently from X-rays and therefore provide information not only on density but also on overall bone quality (Baroncelli 2008). Measurements were performed at the left tibia. The measurement site was standardised at the midpoint between the calcaneus and the superior aspect of the knee joint. Three to five valid SOS measurements were obtained, and the device software automatically generated T- and Z-scores from the obtained values using age-, sex- and ethnicity-specific reference databases. T- and Z-scores are expressed as standard deviations from reference means: the T-score represents deviation from the mean of a young healthy population, while the Z-score represents deviation from the mean of an age- and sex-matched population. According to World Health Organization thresholds (WHO 1994), T-scores is less than or equal to minus 2.5 indicate osteoporosis, values between −1.0 and −2.5 indicate osteopenia and T-score sis greater than or equal to minus 1.0 are considered normal. For Z-scores, values >−2.0 are considered within the expected range for age, whereas Z-scores is less than or equal to minus 2.0 suggest reduced BMD.
Statistical analysis
Statistical analyses were conducted using jamovi (version 2.3.28) and R (version 4.5.1; package snha;(Groth 2023). Normality of distributions was assessed with the Shapiro–Wilk test (α=0.05). For normally distributed variables, independent-samples t tests were used; for non-normal distributions, Mann–Whitney U tests were applied. Season of blood draw was coded by calendar months (winter: Dec–Feb; spring: Mar–May; summer: Jun–Aug; autumn: Sep–Nov) to reflect typical UVB/insolation patterns relevant for vitamin D in Europe (O'Neill et al. 2016). Because data collection took place between February and December 2024, the winter category comprised only February and December samples. One-way Welch ANOVA was used to test the association between season and vitamin D levels. Correlations between allergy categories and bone parameters (Z-score, T-score) at the tibia were evaluated using Pearson’s correlation coefficient. Relationships among variables were explored and mapped using St. Nicolas House Analysis (SNHA; Groth et al. 2019), providing a graph-based visualisation of their associations.
Results
Descriptive characteristics by sex and allergy status are summarized in Table 1 (women) and Table 2 (men). These tables report age, height (cm), body mass (kg), BMI, serum vitamin D (nmol/l) and bone parameters (T-score, Z-score). Among women, vitamin D was lower in the allergic than in the non-allergic group (69.10±26.61 vs 82.89±37.61nmol/l), but the difference was not statistically significant (p=0.108); T- and Z-scores were likewise comparable. Among men, anthropometric measures, vitamin D and bone parameters did not differ between allergic and non-allergic participants. Vitamin D supplementation was not significantly associated with serum vitamin D levels or T- or Z-scores in women or men, and calcium supplementation likewise showed no statistically significant differences in bone quality and quantity or with allergy status. Use of other supplements (vitamin C, B vitamins, magnesium, zinc and multivitamin complexes) did not significantly affect vitamin D levels (all p>0.05).
Table 1 Baseline characteristics of Slovak women by allergy status
Women with allergies (n=97)
Women without allergies (n=48)
Mean
SD
Mean
SD
p
Age
36.24
10.26
35.86
9.63
0.834
Height (cm)
168.06
7.05
168.22
8.15
0.693
Body mass (kg)
71.25
17.85
66.96
12.38
0.323
BMI (kg/m²)
25.23
6.19
23.64
3.98
0.248
Vitamin D (nmol/l)
69.10
26.61
82.89
37.61
0.108
T-score
0.23
1.20
0.54
0.93
0.240
Z-score
0.61
1.20
0.79
0.92
0.400
* Marks statistical significance p<0.05. Abbreviations: n, number of individuals; SD, standard deviation; p, value of statistical significance; BMI, Body mass index.
Table 2 Baseline characteristics of Slovak men by allergy status
Men with allergies (n=37)
Men without allergies (n=16)
Mean
SD
Mean
SD
p
Age
37.55
9.14
34.63
10.73
0.317
Height (cm)
178.44
6.39
178.02
8.48
0.844
Body mass (kg)
84.36
11.99
79.38
11.11
0.162
BMI (kg/m²)
26.45
3.16
25.08
3.32
0.159
Vitamin D (nmol/l)
79.54
35.87
78.66
36.03
0.956
T-score
-0.20
1.01
-0.09
0.91
0.712
Z-score
-0.12
1.00
-0.01
0.92
0.717
* Marks statistical significance p< 0.05. Abbreviations: n, number of individuals; SD, standard deviation; p, value of statistical significance; BMI, Body mass index.
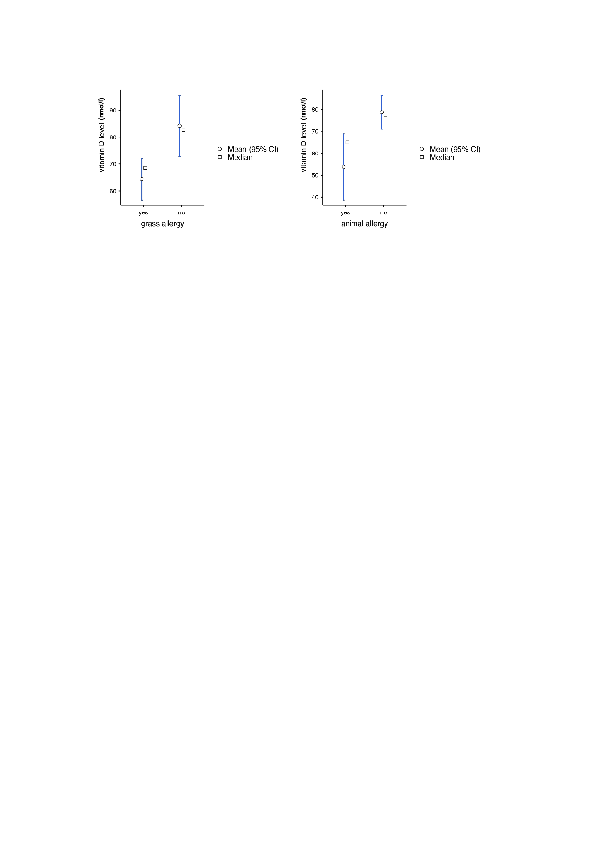
Vitamin D concentrations were significantly lower among women with grasses and animal allergies compared with women without these allergies (grasses: 64.4±24.2 vs 84.2±35.4nmol/l, p=0.006, rrb=0.375; animal: 53.8±27.7 vs 78.7±31.0nmol/l, p=0.011, rrb=0.453). No significant differences were found for food, dust mite, pollen or skin allergies (Table 3). Figure 1 visualises these contrasts, with lower means and medians in the allergy-present groups. In men, vitamin D did not differ across allergy categories (Table 4); analyses used available-case data because several men lacked vitamin D measurements, resulting in smaller subgroup sizes. Welch’s ANOVA found no differences in vitamin D levels across seasons, F(3, 27.1)=2.35, p=0.095. Tukey post hoc comparisons were non-significant (all p is greater than or equal to 0.198).
Table 3 Differences in mean vitamin D levels by allergy category in Slovak women
With allergy
Allergy absent
Type of allergy
n
Mean
SD
n
Mean
SD
p
Rank biserial correlation
Food
15
79.7
28.0
59
72.9
32.7
0.259
0.191
Dust mites
23
68.1
27.3
51
77.1
33.4
0.469
0.107
Pollen
26
70.5
29.0
48
76.4
33.2
0.575
0.080
Grasses
37
64.4
24.2
37
84.2
35.4
0.006*
0.375
Animal
13
53.8
27.7
61
78.7
31.0
0.011*
0.453
Skin allergy
81
75.7
30.8
14
78.6
38.9
0.825
0.038
* Marks statistical significance p<0.05. The rrb effect sizes are calculated using the rank biserial correlation. Abbreviations: n, number of individuals; SD, standard deviation; p, value of statistical significance.
Table 4 Differences in mean vitamin D levels by allergy category in Slovak men
With allergy
Allergy absent
Type of allergy
n
Mean
SD
n
Mean
SD
p
Rank biserial correlation
Food
3
78.9
23.5
18
79.2
37.1
0.814
0.111
Dust mites
7
90.3
39.5
14
73.6
32.7
0.287
0.306
Pollen
8
85.4
38.8
13
75.3
33.5
0.595
0.154
Grasses
8
88.0
39.3
13
73.7
32.5
0.374
0.250
Animal
5
89.5
53.5
16
75.9
28.7
0.548
0.200
Skin allergy
3
96.9
67.6
18
76.4
29.1
0.887
0.074
* Marks statistical significance p<0.05. The rrb effect sizes are calculated using the rank biserial correlation. Abbreviations: n, number of individuals; SD, standard deviation; p, value of statistical significance.
Figure 1 Vitamin D levels (nmol/l) in Slovak women (19–57 years; mean age 36.1±10.0) by allergy status. Panel A: grass allergy (with n=37; without n=37). Panel B: animal allergy (with n=13; without n=61). Abbreviations: CI – confidence interval (created using jamovi version 2.3.28)
Z-scores were significantly lower in women with animal allergy than in those without (0.26±1.14 vs 0.76±1.00; p=0.047; d=0.485) in independent-samples t tests (Table 6). No significant between-group differences were observed for T-scores (Table 5), although contrasts trended lower for pollen (p=0.077), grasses (p=0.085) and animal allergy (p=0.089). For food, dust mites and skin allergy, both T- and Z-scores were comparable between groups.
Table 5 Differences in mean tibial T-score by allergy category in Slovak women
With allergy
Allergy absent
Type of allergy
n
Mean
SD
n
Mean
SD
p
Cohen’s d
Food
17
0.06
0.92
99
0.43
1.06
0.171
0.361
Dust mites
39
0.17
0.93
77
0.48
1.09
0.132
0.298
Pollen
42
0.15
1.18
74
0.51
0.95
0.077
0.345
Grasses
62
0.22
1.11
54
0.56
0.95
0.085
0.323
Animal
21
0.03
1.13
95
0.46
1.02
0.089
0.414
Skin allergy
18
0.42
1.08
98
0.37
1.05
0.873
-0.041
* Marks statistical significance p<0.05. The d-effect sizes are calculated using Cohen's formula. Abbreviations: n, number of individuals; SD, standard deviation; p, value of statistical significance.
Table 6 Differences in mean tibial Z-score by allergy category in Slovak women
With allergy
Allergy absent
Type of allergy
n
Mean
SD
n
Mean
SD
p
Cohen’s d
Food
17
0.38
0.93
99
0.72
1.06
0.228
0.318
Dust mites
39
0.46
0.90
77
0.78
1.09
0.116
0.311
Pollen
42
0.46
1.17
74
0.79
0.95
0.093
0.327
Grasses
62
0.56
1.13
54
0.80
0.92
0.210
0.235
Animal
21
0.26
1.14
95
0.76
1.00
0.047*
0.485
Skin allergy
18
0.67
1.07
98
0.67
1.04
0.989
0.004
* Marks statistical significance p<0.05. The d-effect sizes are calculated using Cohen's formula. Abbreviations: n, number of individuals; SD, standard deviation; p, value of statistical significance.
T- and Z-scores were significantly lower in men with animal allergy than in those without (T-score: −0.78±0.81 vs −0.03±0.96, p=0.035, d=0.798; Z-score: −0.70±0.81 vs 0.05±0.96, p=0.035, d=0.798) in independent-samples t tests (Tables 7–8). No significant differences were observed for food, dust mites, pollen, grasses or skin allergy. Given the small animal-allergy subgroup (n=9 vs 42), these results should be interpreted cautiously and confirmed in larger samples.
* Marks statistical significance p<0.05. The d-effect sizes are calculated using Cohen's formula. Abbreviations: n, number of individuals; SD, standard deviation; p, value of statistical significance.
Table 8 Differences in mean tibial Z-score by allergy category in Slovak men
With allergy
Allergy absent
Type of allergy
n
Mean
SD
n
Mean
SD
p
Cohen’s d
Food
6
-0.28
0.95
45
-0.06
0.98
0.601
0.229
Dust mites
23
0.04
0.93
28
-0.16
1.01
0.550
-0.169
Pollen
26
-0.12
1.13
25
-0.05
0.79
0.807
0.069
Grasses
25
-0.05
1.12
56
-0.12
0.82
0.807
-0.069
Animal
9
-0.70
0.81
42
0.05
0.96
0.035*
0.798
Skin allergy
6
-0.60
1.45
45
-0.02
0.89
0.169
0.607
* Marks statistical significance p<0.05. The d-effect sizes are calculated using Cohen's formula. Abbreviations: n, number of individuals; SD, standard deviation; p, value of statistical significance.
In women, only animal allergy showed a significant negative correlation with the Z-score (p=0.047, r=−0.185) and all T-score correlations were non-significant (Table 9). In men, animal allergy correlated negatively with both T-score (p=0.035, r =−0.297) and Z-score (p=0.035, r=−0.296), whereas other categories showed no associations (Table 10). A negative correlation means that participants with the given allergy tend to have lower T-scores and Z-scores than participants without that allergy, indicating poorer bone quality and quantity.
Table 9 Correlation between bone parameters and allergy categories — Slovak women
Type of allergy:
Food
Dust mites
Pollen
Grasses
Animal
Skin allergy
T-score
r
-0.128
-0.141
-0.165
-0.160
-0.159
0.015
p
0.171
0.132
0.077
0.085
0.089
0.873
n
116
116
116
116
116
116
Z-score
r
-0.113
-0.147
-0.156
-0.117
-0.185
-0.001
p
0.228
0.116
0.093
0.210
0.047*
0.989
n
116
116
116
116
116
116
* Marks statistical significance p<0.05. Abbreviations: r, Pearson’s correlation coefficient; p, value of statistical significance; n, number of individuals.
Table 10 Correlation between bone parameters and allergy categories — Slovak men
Type of allergy:
Food
Dust mites
Pollen
Grasses
Animal
Skin allergy
T-score
r
-0.097
0.084
-0.035
0.040
-0.297
-0.192
p
0.500
0.558
0.805
0.783
0.035*
0.178
n
51
51
51
51
51
51
Z-score
r
-0.075
0.086
-0.035
0.035
-0.296
-0.196
p
0.601
0.550
0.807
0.807
0.035*
0.169
n
51
51
51
51
51
51
* Marks statistical significance p<0.05. Abbreviations: r, Pearson’s correlation coefficient; p, value of statistical significance; n, number of individuals.
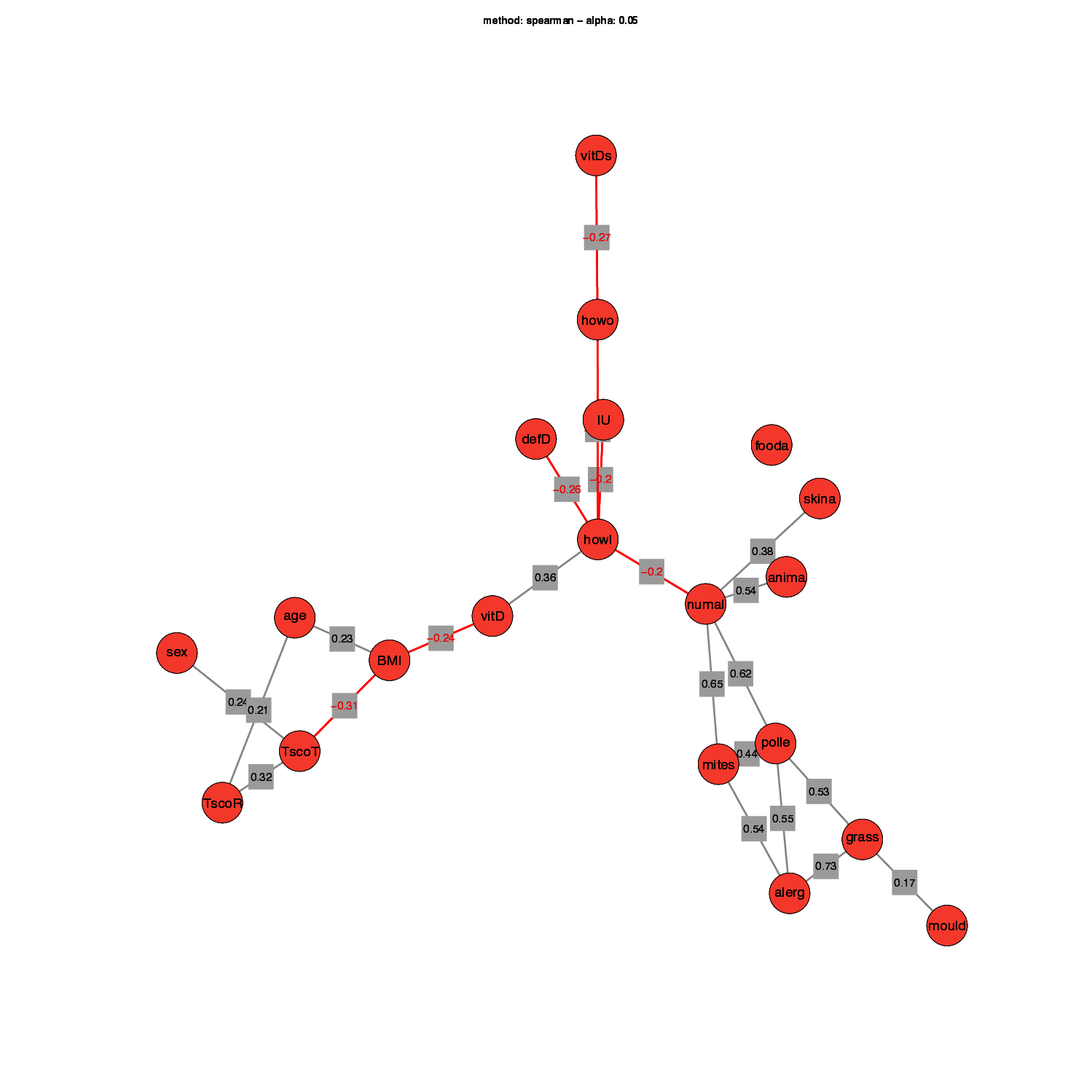
Finally, to summarise the relationships between variables, we used SNHA (Figure 2). SNHA highlights the links among three areas of variables. On the left is the anthropometric area with age, sex, BMI and T-scores. In the middle is the vitamin D area with vitamin D levels and supplementation variables. On the right is the allergy area with the specific allergy categories and the number of allergy types. Vitamin D relates to T-scores indirectly through BMI, because BMI correlates negatively with vitamin D and with T-scores. The allergy area connects to vitamin D, and the duration of vitamin D use is negatively associated with the number of allergy types.
Figure 2 SNHA of bone parameters, vitamin D and allergy categories in Slovak adults. Abbreviations: TscoR, T-score radius; TscoT, T-score tibia; BMI, body mass index; vitD, vitamin D levels; vitDs, vitamin D supplements; howo, how often does one take vit D; howl, how long does one take vit D; IU, how many units of vit D does one have; defD, whether one has ever been found to be deficient in vit D; numal, the number of allergy types; fooda, food allergy; skina, skin allergy; anima, allergy to animals; mites, allergy to mites; pollen, allergy to pollen; grass, grass allergy; mould, mould allergy (created using R version 4.5.1–Package snha (Groth 2023))
Discussion
This study examined the associations between physician-diagnosed allergy categories and the quality and quantity of bone tissue, assessed using QUS at the tibia. Another aim was to assess whether vitamin D levels differ by allergy status. Among women, vitamin D levels were lower in those with grass and animal allergies, whereas no differences were observed in other allergy categories. This pattern supports our second hypothesis in women, that allergic individuals would have lower vitamin D, while it was not observed in men. These findings are consistent with several studies reporting lower serum 25(OH)D concentrations in patients with allergic rhinitis (Kajal et al. 2022; Ma et al. 2020; Saad et al. 2020), although evidence across populations remains heterogeneous.
Several studies in adult populations have not demonstrated consistent associations between serum 25(OH)D and allergic diseases. In a large prospective cohort of 4,999 Danish adults, with baseline 25(OH)D measured using a chromatography-based method, no significant associations were found between baseline 25(OH)D and atopy or doctor-diagnosed asthma, suggesting that vitamin D status may not be a major determinant of allergy onset in adulthood (Thuesen et al. 2015). In a smaller case–control study of Chinese adults with persistent allergic rhinitis (32 patients) and non-allergic controls (25 individuals), serum 25(OH)D measured by ELISA did not differ significantly between groups, although within the allergic group vitamin D was inversely associated with blood eosinophil counts, indicating a closer link with inflammatory activity than with the presence of the disease itself (Wu et al. 2017b). Consistent with this, an Italian cross-sectional multicentre survey of 309 adults with confirmed allergic diseases, in which 25(OH)D was assessed using commercial ELISA kits, found no overall association between vitamin D levels and respiratory allergy, but detected signals for perennial allergens (house dust mites, dog dander) and atopic dermatitis (Lombardi et al. 2017). These discrepancies compared with our findings, where lower 25(OH)D was observed in women with grass and animal allergies, may reflect differences in study design (prospective cohort vs cross-sectional and case–control designs), in sample size (large population-based cohorts vs smaller clinical samples), in the outcomes examined (physician-diagnosed asthma or rhinitis versus allergen-specific categories), in population characteristics (Danish, Chinese and Italian samples versus an adult Central European outpatient population) and in the laboratory methods used to quantify serum 25(OH)D. Taken together, these observations underline that the relationship between vitamin D status and allergy is likely complex and context dependent rather than uniform across all phenotypes and populations.
In contrast, no significant differences in vitamin D levels were observed among men across allergy categories. This likely reflects reduced statistical power, given the smaller male subgroup sizes and missing vitamin D measurements, which may have limited our ability to detect subtle associations. These findings collectively add to the evidence that vitamin D status may be linked to allergic conditions and may be modulated by sex (Zhang et al. 2024). In our sample, vitamin D also did not vary by season of blood draw, reducing concern about seasonal sampling effects.
In women, comparisons across allergy categories and correlation analyses pointed in the same direction. Across both sexes, animal allergy emerged as the only category consistently associated with poorer bone parameters, showing lower T- and/or Z-scores and negative correlations with these measures in women and men. These results partially support our first hypothesis—that adults with allergies would show lower bone tissue quality and quantity, as the effects were limited to animal allergy and differed by sex. Animal allergy is a known trigger of allergic rhinitis, and exposure to animal allergens has been associated with an increased risk of developing asthma (Bjerg et al. 2015; Takkouche et al. 2008). Mechanistically, chronic inflammation in allergic and autoimmune disorders disrupts bone remodelling, shifting the balance from formation to resorption and increasing the risk of osteoporosis (Ginaldi and Martinis 2016). However, not all evidence points to increased osteoporosis risk: in patients with chronic rhinosinusitis with nasal polyposis undergoing long-term corticosteroid therapy, the prevalence of osteopenia/osteoporosis was comparable to that in controls, and no within-group predictors of bone metabolism alterations were identified (Gelardi et al. 2019). At the population level, a large Korean study (n = 162,579 adults) found that asthma was associated with higher odds of osteoporosis. The risk showed a disease-control gradient—lower in well-controlled and treated asthma and highest in untreated asthma—with consistent associations in women and the strongest effect in untreated men (Wee et al. 2020). Similarly, a case–control analysis observed elevated osteoporosis risk in adults with chronic rhinosinusitis, not clearly attributable to medication exposure (Choi and Kong 2019).
Linking these findings, allergy, vitamin D and the skeletal system may be connected through shared biological mechanisms, with vitamin D acting as an immunomodulatory bridge between allergic pathways and skeletal remodelling and with allergy mediators such as histamine influencing osteoclastogenesis (Ginaldi and Martinis 2016; Sirufo et al. 2020). In addition to these biological pathways, behavioural mechanisms may also contribute to the observed associations. Individuals with grass allergy are often advised to limit outdoor exposure during periods of high pollen levels, which may reduce cutaneous vitamin D synthesis and opportunities for weight-bearing activity, particularly from spring to autumn. Epidemiological data in allergic rhinitis populations indicate that allergic disease can impair daily activities and is frequently associated with reduced outdoor activity and participation in physical exercise (Alblewi et al. 2024). In our sample, however, self-reported sport frequency and type of physical activity did not differ meaningfully between allergic and non-allergic participants and showed no clear relationship with T- or Z-scores or vitamin D levels. Within the limits of our measures and sample size, we therefore did not observe evidence that physical activity explained the associations between allergy, vitamin D and bone parameters. Nevertheless, the absence of a detectable effect in our data does not rule out more subtle or seasonal differences in outdoor exposure, and future studies should incorporate more detailed and objective assessments of physical activity and sun exposure. In our data, women with grasses and animal allergies had lower vitamin D and animal allergy was associated with lower bone tissue quality and quantity in sex-specific analyses. SNHA summarised the correlation structure as chains of associations and, in our data, supported indirect connections among allergy, vitamin D and bone (notably via BMI and supplementation) rather than a single direct link.
In summary, sex-specific analyses indicated that selected allergy categories, in particular animal allergy, were associated with poorer bone parameters and that women with grass and animal allergies had lower vitamin D levels than women without these allergies. No seasonal effects on vitamin D were observed. Several factors may underlie these sex- and allergy-specific patterns. At a biological level, chronic inflammation associated with allergic disease and the release of mediators such as histamine and cytokines may promote bone resorption and impair bone formation, particularly in individuals with more persistent allergic disease (Sirufo et al. 2020). In addition, lower vitamin D levels in women with grass and animal allergies may reflect a combination of immunological mechanisms and behavioural adaptations, such as limiting outdoor activities during pollen seasons, which could reduce cutaneous vitamin D synthesis and exposure to weight-bearing activity (Lu et al. 2025; Zhang et al. 2024). The absence of seasonal variation in vitamin D in our sample suggests that these differences are unlikely to be driven solely by the timing of blood sampling and may instead relate to more stable individual differences in lifestyle, body composition and disease burden. Consistent with this, studies in children have shown that lower outdoor activity is associated with a higher risk of asthma and allergic rhinitis, pointing to behavioural pathways linking allergy, environment and health (Lu et al. 2025). Finally, the fact that the differences were more apparent in women than in men may reflect sex-related differences in bone turnover, hormonal status and body composition (Chen et al. 2025), as well as lower statistical power in the male subsample. Together, these considerations support a multifactorial interpretation in which allergic status, vitamin D and bone health are linked through a combination of biological, behavioural, and contextual factors rather than a single isolated mechanism.
Study limitations
This study is observational and cross-sectional, so causality cannot be inferred. The sample was modest and sex-imbalanced (145 women, 53 men), with small allergy-specific subgroups and missing vitamin D data in men. Analyses used available cases, which reduces statistical power and may introduce bias. Participants were recruited from a single outpatient clinic, which may limit generalisability. Moreover, medication exposures, menopausal status and biochemical markers of bone metabolism (e.g., PTH, calcium) were not accounted for, which could confound or mediate the observed associations. Additionally, individual exposure to sunlight such as time spent outdoors, clothing habits and sunscreen use was not assessed, which limits the ability to account for variability in endogenous vitamin D synthesis.
Despite these limitations, the study has several strengths. Allergy status was based on physician-diagnosed categories rather than self-report alone, and bone parameters were assessed using a validated QUS device at the tibia. The combined assessment of allergy status, vitamin D levels and bone parameters in an adult Central European outpatient population, together with sex-specific analyses, provides clinically relevant insight into potential links between allergic disease and bone health.
Conclusion
Our study points to a link between allergy categories and bone tissue quality and quantity. In sex-specific analyses, animal allergy was associated with lower bone parameters (women: lower Z-scores; men: lower T- and Z-scores), and women with grass and animal allergies had lower vitamin D than women without these allergies. Vitamin D did not vary by season. SNHA suggested indirect connections among allergy, vitamin D and bone tissue quality and quantity. These findings warrant attention to vitamin D status and monitoring of bone tissue quality and quantity in adults with relevant allergies, and they call for larger, sex-balanced longitudinal studies. Based on these findings, it may be appropriate to consider more frequent monitoring of vitamin D levels in adults with allergic disease so that any deficiency can be detected early and corrected as needed. In individuals with allergies and additional risk factors for osteoporosis, periodic assessment of bone status may also be warranted, following consultation with a physician.
Authors contribution
Alexandra Hozáková collected data, performed the statistical analyses and drafted the manuscript. Lenka Vorobeľová and Darina Falbová designed the study and revised and edited the manuscript. Veronika Mundoková Csibová provided clinical oversight, facilitated patient recruitment and data collection in the outpatient clinic and verified allergy diagnoses. Simona Sulis contributed to data collection and manuscript writing. All authors read and approved the final version of the manuscript.
Acknowledgements
We gratefully acknowledge Prof. Dr. Christiane Scheffler, Prof. Dr. Michael Hermanussen and Dr. Detlef Groth for their insightful advice on study design and data analysis during the 8th Summer School “Human Growth and Development—Data Analysis and Statistics” (Gülpe, Germany, 2025), organised with KoUP funding support from the University of Potsdam. We also thank RNDr. Petra Švábová, PhD. for facilitating the introduction to Dr. Veronika Mundoková, which enabled patient recruitment and measurements in the outpatient clinic. This work was supported by the Ministry of Education, Science, Research and Sport of the Slovak Republic funded the study, Grant/Award Number: KEGA 046UK-4/2023 and Grant/Award Number: UK/1017/2025.
References
Alblewi, S. M. S./Alenazi, L. M./Alshahrani, R. S./Alharbi, R. T./Alotaibi, N. A./Albalawi, H. M. D./Albalawi, D. L. S./Alfaidi, A. A./Abu Sabir, D. A. H. (2024). Prevalence of Allergic Rhinitis and its Impact on Quality of Life Among Pediatric Patients in Tabuk, Saudi Arabia. Oman medical journal 39 (6), e696. https://doi.org/10.5001/omj.2024.118.
Baroncelli, G. I. (2008). Quantitative ultrasound methods to assess bone mineral status in children: technical characteristics, performance, and clinical application. Pediatric Research 63 (3), 220–228. https://doi.org/10.1203/PDR.0b013e318163a286.
Bjerg, A./Winberg, A./Berthold, M./Mattsson, L./Borres, M. P./Rönmark, E. (2015). A population‐based study of animal component sensitization, asthma, and rhinitis in schoolchildren. Pediatric Allergy and Immunology 26 (6), 557–563. https://doi.org/10.1111/pai.12422.
Bora, S. A./Kennett, M. J./Smith, P. B./Patterson, A. D./Cantorna, M. T. (2018). Regulation of vitamin D metabolism following disruption of the microbiota using broad spectrum antibiotics. The Journal of Nutritional Biochemistry 56, 65–73. https://doi.org/10.1016/j.jnutbio.2018.01.011.
Bouillon, R./Marcocci, C./Carmeliet, G./Bikle, D./White, J. H./Dawson-Hughes, B./Lips, P./Munns, C. F./Lazaretti-Castro, M./Giustina, A./Bilezikian, J. (2019). Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding Questions. Endocrine Reviews 40 (4), 1109–1151. https://doi.org/10.1210/er.2018-00126.
Chen, S./Patel, J./Katzmeyer, T./Pei, M. (2025). Sex-dependent variation in bone adaptation: from degeneration to regeneration. Journal of Orthopaedic Translation 52, 325–343. https://doi.org/10.1016/j.jot.2025.04.011.
Choi, H. G./Kong, I. G. (2019). Association between chronic rhinosinusitis and osteoporosis: a case‐control study using a national sample cohort. International Forum of Allergy & Rhinology 9 (9), 1010–1016. https://doi.org/10.1002/alr.22365.
Doulgeraki, A. E./Manousakis, E. M./Papadopoulos, N. G. (2017). Bone health assessment of food allergic children on restrictive diets: a practical guide. Journal of Pediatric Endocrinology and Metabolism 30 (2). https://doi.org/10.1515/jpem-2016-0162.
Douros, K./Loukou, I./Boutopoulou, B./Fouzas, S. (2015). Does Vitamin D Deficiency Epidemic Parallel with Allergy and Asthma Epidemic? Mini-Reviews in Medicinal Chemistry 15 (12), 967–973. https://doi.org/10.2174/138955751512150731110827.
Gelardi, M./Barbara, F./Covelli, I./Damiani, M. A./Plantone, F./Notarnicola, A./Moretti, B./Quaranta, N./Ciprandi, G. (2019). Long-Term Therapy with Corticosteroids in Nasal Polyposis: A Bone Metabolism Assessment. Indian Journal of Otolaryngology and Head & Neck Surgery 71 (Suppl 3), 2050–2056. https://doi.org/10.1007/s12070-018-1466-5.
Groth, D. (2023). GitHub –mittelmark/snha:St. Nicolas House Algorithm implementation in R –predicting correlation networks using association chains 2023. Available online at https://github.com/mittelmark/snha.
Groth, D./Scheffler, C./Hermanussen, M. (2019). Body height in stunted Indonesian children depends directly on parental education and not via a nutrition mediated pathway – Evidence from tracing association chains by St. Nicolas House Analysis. Anthropologischer Anzeiger 76 (5), 445–451. https://doi.org/10.1127/anthranz/2019/1027.
Jung, J.-W./Kang, H.-R./Kim, J.-Y./Lee, S.-H./Kim, S. S./Cho, S. H. (2014). Are asthmatic patients prone to bone loss? Annals of Allergy, Asthma & Immunology 112 (5), 426–431. https://doi.org/10.1016/j.anai.2014.02.013.
Kajal, S./Shrestha, P./Gupta, Y./Deepak, R./Verma, H. (2022). Vitamin D Deficiency and Interleukin Levels in Allergic Rhinitis: A Case–Control Study. Indian Journal of Otolaryngology and Head & Neck Surgery 74 (Suppl 2), 1720–1724. https://doi.org/10.1007/s12070-021-02897-y.
Krajewska, M./Witkowska-Sędek, E./Rumińska, M./Stelmaszczyk-Emmel, A./Sobol, M./Majcher, A./Pyrżak, B. (2022). Vitamin D Effects on Selected Anti-Inflammatory and Pro-Inflammatory Markers of Obesity-Related Chronic Inflammation. Frontiers in Endocrinology 13, 920340. https://doi.org/10.3389/fendo.2022.920340.
Laird, E./Ward, M./McSorley, E./Strain, J. J./Wallace, J. (2010). Vitamin D and Bone Health; Potential Mechanisms. Nutrients 2 (7), 693–724. https://doi.org/10.3390/nu2070693.
Lipińska-Opałka, A./Tomaszewska, A./Kubiak, J. Z./Kalicki, B. (2021). Vitamin D and Immunological Patterns of Allergic Diseases in Children. Nutrients 13 (1), 177. https://doi.org/10.3390/nu13010177.
Lohman, T. G./Roche, A. F./Martorell, R. (1988). Anthropometric standardization reference manual. Champaign, Ill., Human Kinetics Books.
Lombardi, C./Passalacqua, G./Italian Vitamin D Allergy Group (2017). Vitamin D levels and allergic diseases. An italian cross-sectional multicenter survey. European Annals of Allergy and Clinical Immunology 49 (2), 75–79.
Lu, R./Zhang, Y./Chen, Y./Lyu, J./Li, R./Kang, W./Zhao, A./Ning, Z./Hu, Y./Lin, X./Tong, S./Lu, Z./Li, S. (2025). The Joint Association of Sleep Quality and Outdoor Activity with Asthma and Allergic Rhinitis in Children: A Cross-Sectional Study in Shanghai. Journal of Asthma and Allergy 18, 101–111. https://doi.org/10.2147/JAA.S494662.
Ma, Y./Liu, Y./Li, X./Qiu, J./Fang, P. (2020). Low serum 25‐hydroxyvitamin D levels are associated with perennial allergic rhinitis but not disease severity. Journal of Clinical Laboratory Analysis 34 (12), e23516. https://doi.org/10.1002/jcla.23516.
Martinis, M. de/Allegra, A./Sirufo, M. M./Tonacci, A./Pioggia, G./Raggiunti, M./Ginaldi, L./Gangemi, S. (2021). Vitamin D Deficiency, Osteoporosis and Effect on Autoimmune Diseases and Hematopoiesis: A Review. International Journal of Molecular Sciences 22 (16), 8855. https://doi.org/10.3390/ijms22168855.
Martinis, M. de/Sirufo, M. M./Ginaldi, L. (2020). Osteoporosis: Current and Emerging Therapies Targeted to Immunological Checkpoints. Current Medicinal Chemistry 27 (37), 6356–6372. https://doi.org/10.2174/0929867326666190730113123.
Mirzakhani, H./Al‐Garawi, A./Weiss, S. T./Litonjua, A. A. (2015). Vitamin D and the development of allergic disease: how important is it? Clinical & Experimental Allergy 45 (1), 114–125. https://doi.org/10.1111/cea.12430.
Murdaca, G./Allegra, A./Tonacci, A./Musolino, C./Ricciardi, L./Gangemi, S. (2022). Mast Cells and Vitamin D Status: A Clinical and Biological Link in the Onset of Allergy and Bone Diseases. Biomedicines 10 (8), 1877. https://doi.org/10.3390/biomedicines10081877.
Mvoundza Ndjindji, O./Minto’o Rogombe, S./Mveang-Nzoghe, A./Leboueny, M./Ouloungou, M./Abougono Ekogha, N./Maloupazoa Siawaya, A. C./Kuissi Kamgaing, É./Ndeboko, B./Ategbo, S./Djoba Siawaya, J. F. (2024). Vitamin D deficiency may be associated with allergies in sub-Saharan Africa. Journal of Allergy and Hypersensitivity Diseases 2, 100011. https://doi.org/10.1016/j.jahd.2024.100011.
O'Neill, C. M./Kazantzidis, A./Ryan, M. J./Barber, N./Sempos, C. T./Durazo-Arvizu, R. A./Jorde, R./Grimnes, G./Eiriksdottir, G./Gudnason, V./Cotch, M. F./Kiely, M./Webb, A. R./Cashman, K. D. (2016). Seasonal Changes in Vitamin D-Effective UVB Availability in Europe and Associations with Population Serum 25-Hydroxyvitamin D. Nutrients 8 (9). https://doi.org/10.3390/nu8090533.
Ponzetti, M./Rucci, N. (2019). Updates on Osteoimmunology: What’s New on the Cross-Talk Between Bone and Immune System. Frontiers in Endocrinology 10, 236. https://doi.org/10.3389/fendo.2019.00236.
Rueter, K./Siafarikas, A./Palmer, D. J./Prescott, S. L. (2022). Pre- and Postnatal Vitamin D Status and Allergy Outcomes in Early Childhood. Biomedicines 10 (5), 933. https://doi.org/10.3390/biomedicines10050933.
Saad, K./Abdelmoghny, A./Aboul-Khair, M. D./Abdel-Raheem, Y. F./Gad, E. F./Hammour, A. E.-S./Hawary, B./Zahran, A. M./Alblihed, M. A./Elhoufey, A. (2020). Vitamin D Status in Egyptian Children With Allergic Rhinitis. Ear, Nose & Throat Journal 99 (8), 508–512. https://doi.org/10.1177/0145561319850814.
Sirufo, M. M./Suppa, M./Ginaldi, L./Martinis, M. de (2020). Does Allergy Break Bones? Osteoporosis and Its Connection to Allergy. International Journal of Molecular Sciences 21 (3), 712. https://doi.org/10.3390/ijms21030712.
Takkouche, B./González‐Barcala, F.-J./Etminan, M./FitzGerald, M. (2008). Exposure to furry pets and the risk of asthma and allergic rhinitis: a meta‐analysis. Allergy 63 (7), 857–864. https://doi.org/10.1111/j.1398-9995.2008.01732.x.
Thuesen, B. H./Skaaby, T./Husemoen, L. L. N./Fenger, M./Jørgensen, T./Linneberg, A. (2015). The association of serum 25-OH vitamin D with atopy, asthma, and lung function in a prospective study of Danish adults. Clinical & Experimental Allergy 45 (1), 265–272. https://doi.org/10.1111/cea.12299.
Wang, J./Zhou, Y./Zhang, H./Hu, L./Liu, J./Wang, L./Wang, T./Zhang, H./Cong, L./Wang, Q. (2023). Pathogenesis of allergic diseases and implications for therapeutic interventions. Signal Transduction and Targeted Therapy 8 (1), 138. https://doi.org/10.1038/s41392-023-01344-4.
Wee, J. H./Min, C./Park, M. W./Byun, S. H./Lee, H.-J./Park, B./Choi, H. G. (2020). The association of asthma and its subgroups with osteoporosis: a cross-sectional study using KoGES HEXA data. Allergy, Asthma & Clinical Immunology 16 (1), 84. https://doi.org/10.1186/s13223-020-00482-6.
Wu, C.-Y./Lu, Y.-Y./Lu, C.-C./Su, Y.-F./Tsai, T.-H./Wu, C.-H./van Nguyen, T. (2017a). Osteoporosis in adult patients with atopic dermatitis: A nationwide population-based study. PLOS One 12 (2), e0171667. https://doi.org/10.1371/journal.pone.0171667.
Wu, H.-Y./Chen, J.-X./Tian, H.-Q./Zhang, X.-L./Bian, H.-Y./Cheng, L. (2017b). Serum 25-hydroxyvitamin D inversely associated with blood eosinophils in patients with persistent allergic rhinitis. Asia Pacific Allergy 7 (4), 213–220. https://doi.org/10.5415/apallergy.2017.7.4.213.
Zhang, P./Xu, Q./Zhu, R. (2024). Vitamin D and allergic diseases. Frontiers in Immunology 15, 1420883. https://doi.org/10.3389/fimmu.2024.1420883.
 ✉
✉